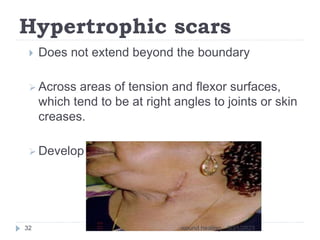
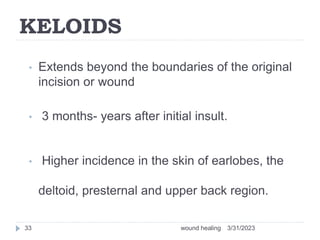
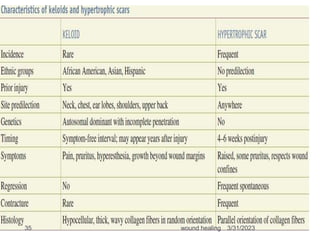
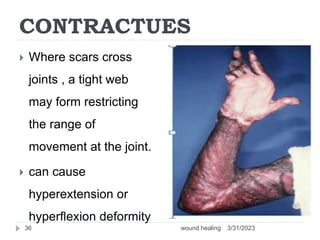
This document provides an overview of wound healing and classification. It discusses the phases of wound healing including hemostasis and inflammation, proliferative phase, and maturation and remodeling. Factors affecting wound healing and healing in specific tissues like bone, cartilage, and nerves are also reviewed. Chronic wounds like ischemic, venous stasis, diabetic and pressure ulcers are described. Excess healing processes such as hypertrophic scarring, keloids, and contractures are also summarized.