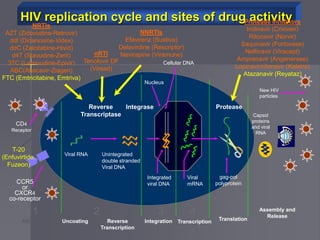
This document discusses the various skin manifestations that can occur in patients with HIV/AIDS. It notes that up to 92% of patients will experience one or more skin disorders throughout their illness. Conditions range from common issues like seborrheic dermatitis and xerosis to more specific diseases such as Kaposi's sarcoma, bacillary angiomatosis, and oral hairy leukoplakia. Bacterial, viral, and fungal infections are also more frequent and severe in immunocompromised HIV/AIDS patients. Recognizing cutaneous signs of HIV can lead to earlier diagnosis and treatment.
































































































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)















