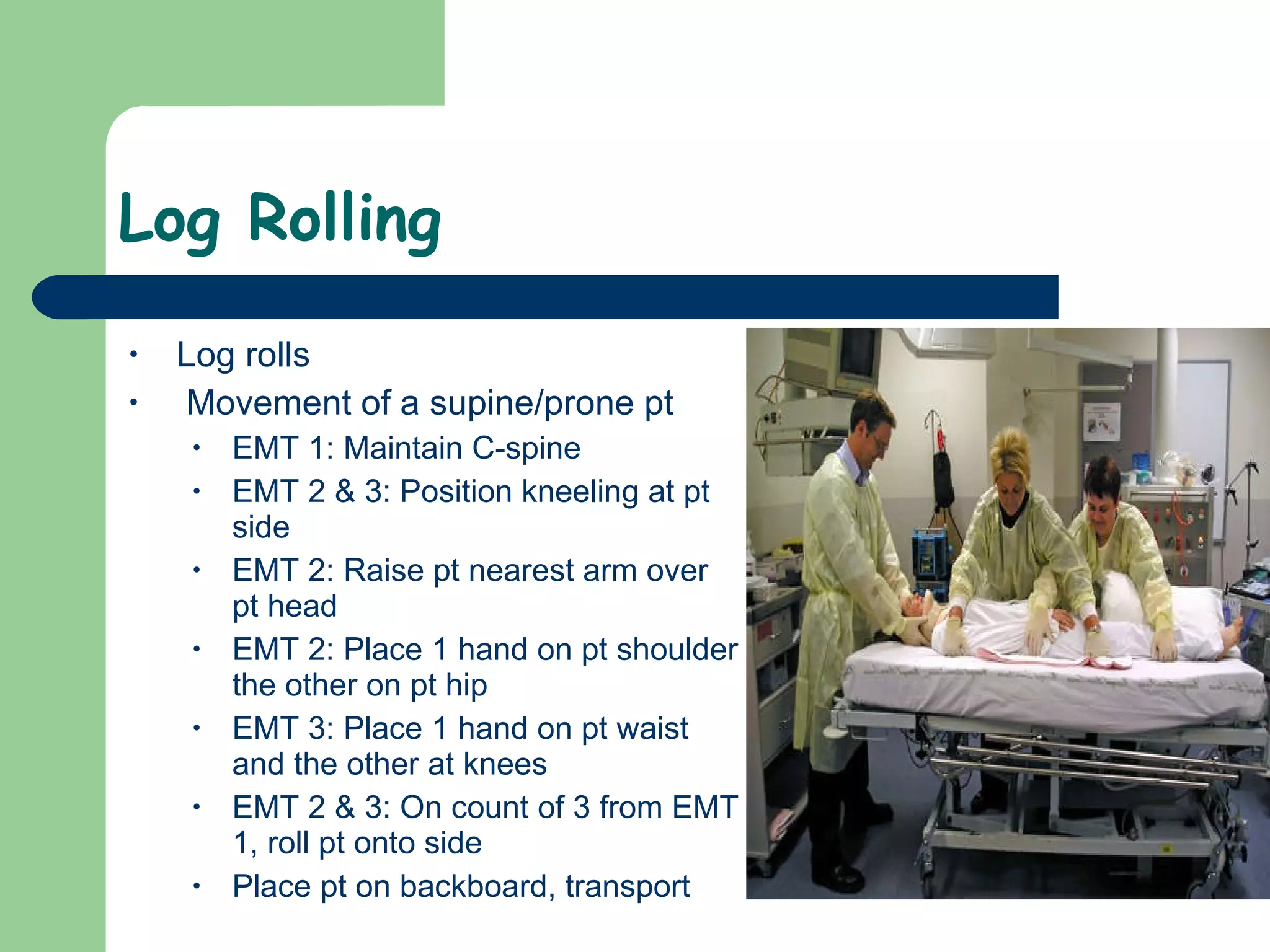
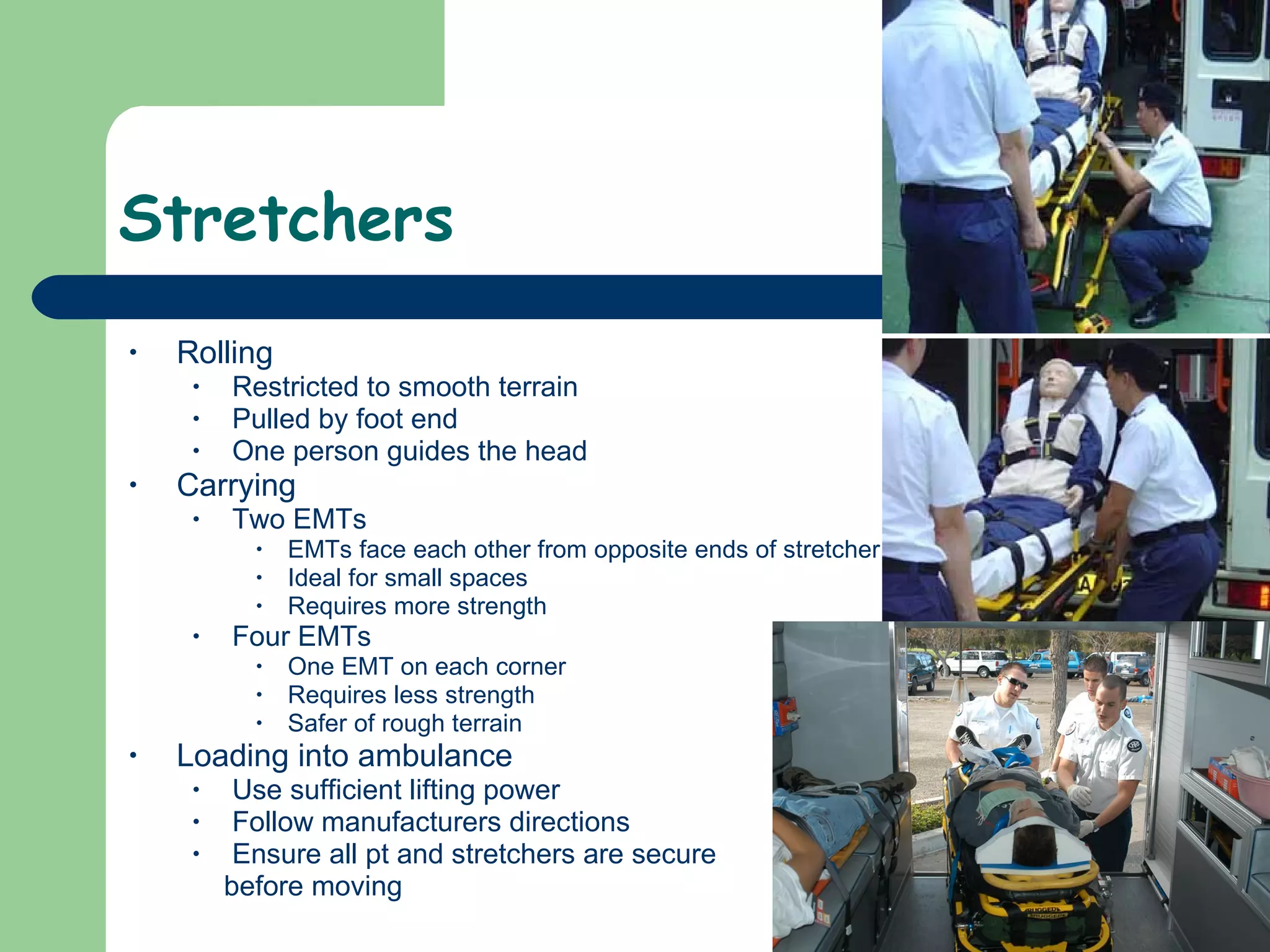
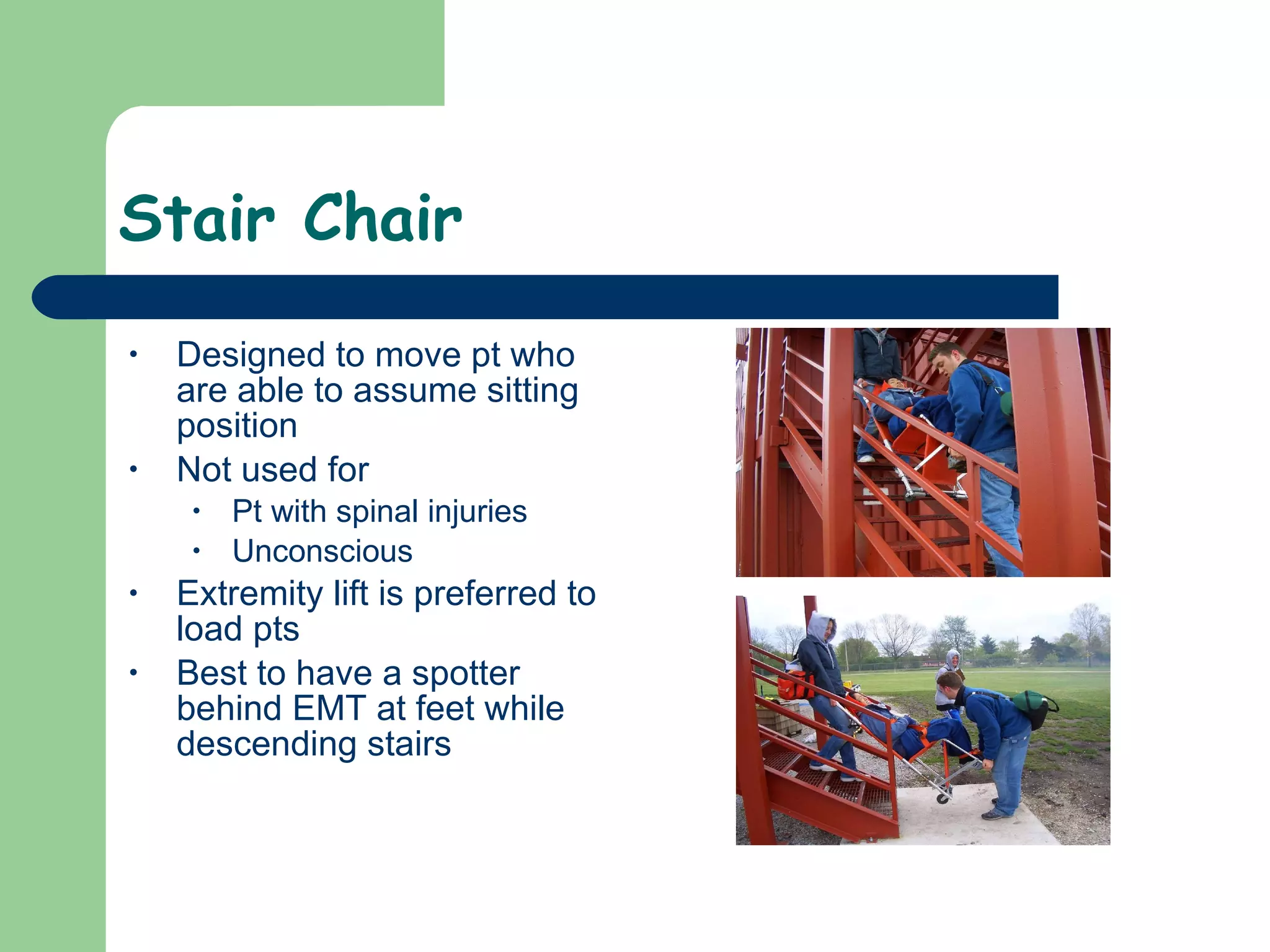
Body mechanics and safety precautions are important when lifting and moving patients to prevent injury. Techniques include using legs instead of back to lift, keeping the weight close, and avoiding twisting motions. Patients should be lifted based on their condition, from emergency moves for imminent danger to non-urgent moves for stable patients. Various devices like backboards, stretchers, stair chairs, and scoops can be used to safely transport patients.