
Downloaded 827 times
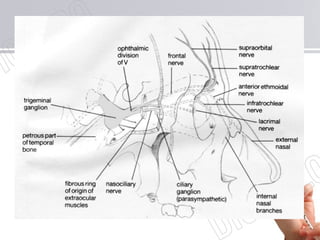
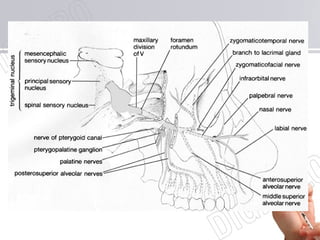
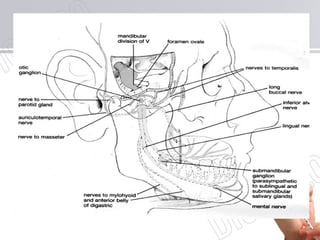
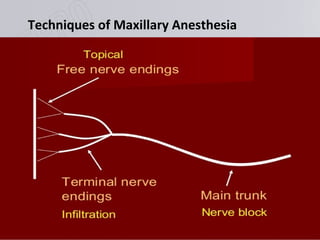
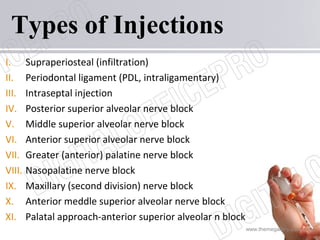


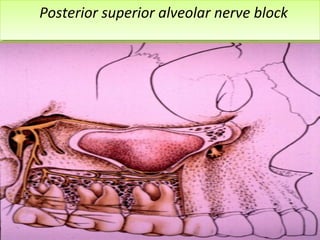
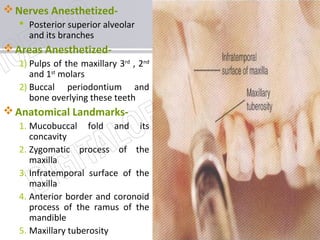

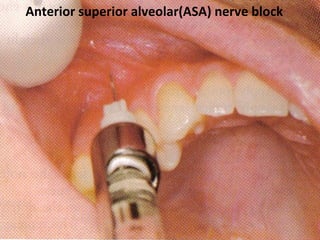
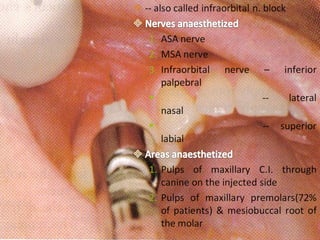
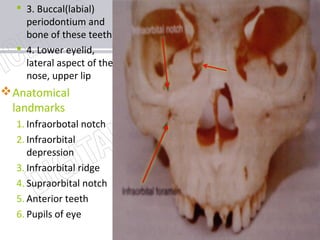
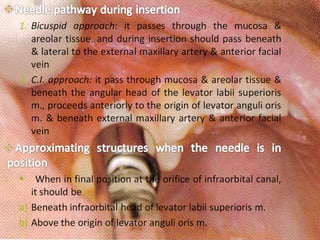

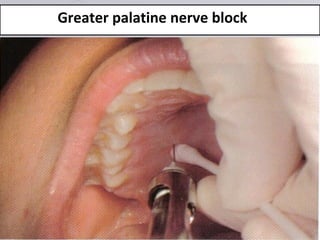
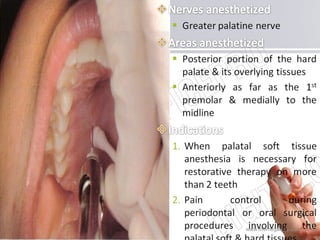
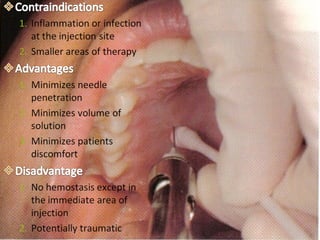
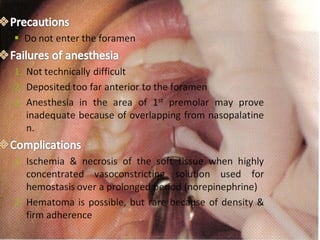
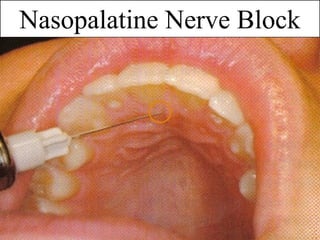

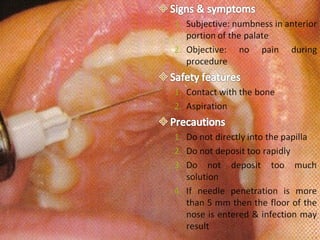
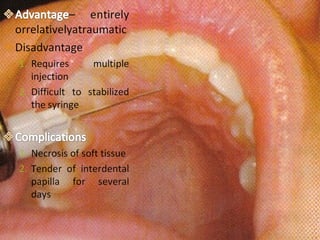
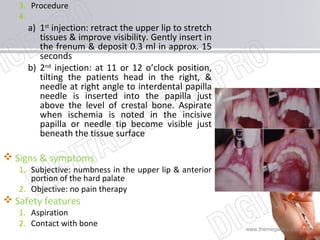
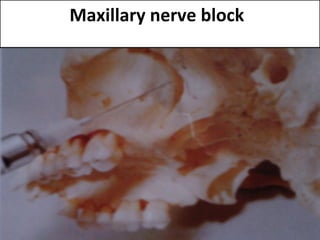
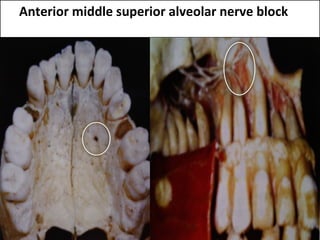
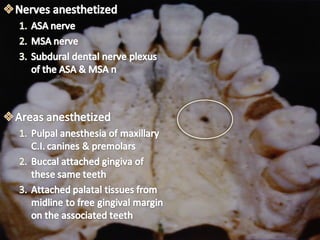
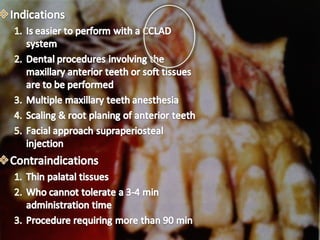
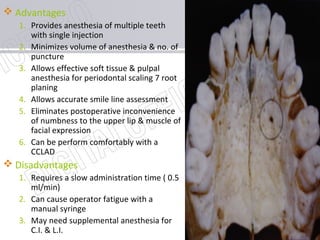
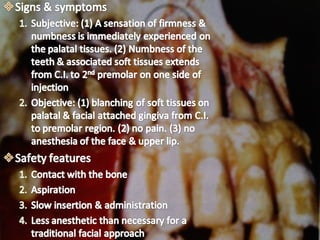

This document discusses various techniques for maxillary nerve blocks and anesthesia. It begins by outlining the maxillary nerve and its branches, then describes 10 different injection techniques in detail. These include supraperiosteal, posterior superior alveolar, anterior superior alveolar, middle superior alveolar, greater palatine, nasopalatine, and maxillary nerve blocks. Each technique section explains the nerves anesthetized, areas anesthetized, anatomical landmarks, advantages and disadvantages, and procedural steps. Images are provided to illustrate the injection sites and anatomical relationships.






























![Techniques of local anesthesia [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/techniquesoflocalanesthesiaautosaved-210618141111-thumbnail.jpg?width=640&height=640&fit=bounds)
























































