
Downloaded 47 times

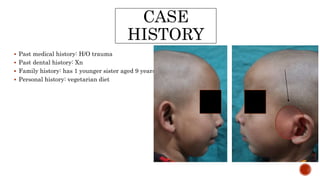
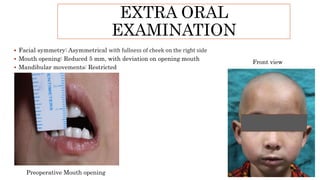
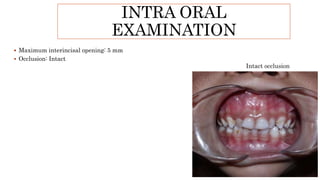
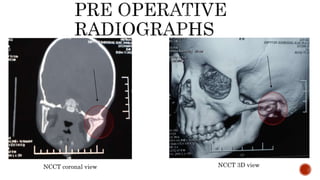
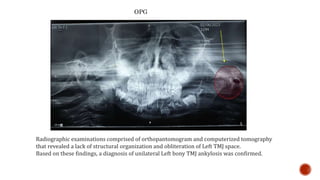
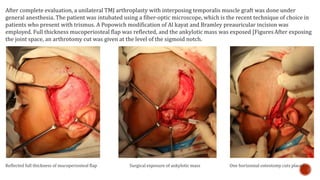
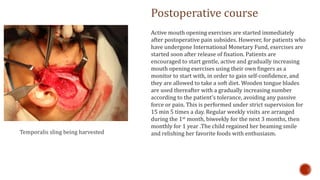

A 5-year-old female child presented with inability to open her mouth for 1 month due to trauma sustained 13 months prior. Clinical examination and radiographic imaging revealed a lack of structural organization and obliteration of the left temporomandibular joint (TMJ) space, confirming a diagnosis of unilateral left bony TMJ ankylosis. The patient underwent a unilateral TMJ arthroplasty with an interposing temporalis muscle graft under general anesthesia. Postoperatively, active mouth opening exercises were started to regain mouth opening. At follow-up, the child had regained her smile and ability to enjoy favorite foods.























































































