
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Head injury
Similar to Head injury (20)
More from M Ridhwan Abd Razak
More from M Ridhwan Abd Razak (20)
Recently uploaded
Recently uploaded (20)
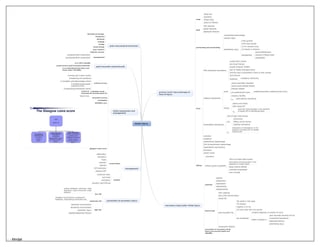
Head injury
- 1. Head injury primary brain injury:damage at time of injury scalp blood loss laceration foreign body portal of infection skull liner fractures basilar fractures depressed fractures perforating and penetrating intracerebral haemorrhage vascular injury penetrating injury 4.6% gunshot 0.4% stab wounds 1/3 hv vascular injury 1/3 results in infection management wound debridement removal of foreign body angiography focal EDH=extradural haematoma usually blunt trauma a/w linear fracture usually temporal 70-80% tear of middle meningeal artery biconvex due to attachment of dura to skull sutures lucid interval treatment emergency craniotomy subdural haematoma acute venous tear/brain laceration covers entire cerebral surface srescent shaped a/w parenchymal injury morbidity/mortality underlying brain injury mortality 30-90% tx early elective craniotomy chronic elderly and infants 50% raised ICP Tx early burr hole drainage in the presence of raised ICP of lateralising signs intracerebral haematoma 15% of fatal head injuries a/w contussions diffuse axonal injuries subdural haematoma Tx evacuation of haematoma in the presence of raised ICP or marked midline shift contusion laceration subarachnoid haemorrhage IVH=intraventricular haemorrhage hypothalamic and pituitary brainstem cranial nerves diffuse concussion diffuse axonal injury(DAI) 35% of all fatal head injuries prolonged unconsciousness in the absence of a mass lesion basal cisterns effaced ventricles compressed sulci invisible secondary injury:after initial injury systemic hypoxia hypotension hypercapnia hyperthermia hypoglycaemia intracranial brain swelling brain shift and herniation raised ICP post-traumatic fits 5% adults in first week 7% children majority in 24 hrs 2/3 have more than one seizure can be delayed incidence depends on severity of injury higher incidence if post traumatic amnesia>24 hrs intracranial haematoma depressed fracture penetrating injury intracranial infection prevention of secondary brain injury can prevent death and disability prevention of secondary injury low risk asymp, headache, dizziness, scalp laceration, scalp contussion, scalp abrasion moderate risk changeof consciousness, progressive headache, alcohol/drug intoxication etc high risk depressed consciousness decreasing consciousness penetratin injury palpable/depressed fracture management conservative observation ventilation fluids mannitol steroids ICP monitoring maintain CPP surgical ventricular drain burr holes craniotomy elevation skull fracture initial assessment and management primary survey A-airway and C-spine control B-breathing and ventilation C-circulation and ahemorrhage control D-disability(neurological evaluation-GCS) E-exposure/environmental control if GCS<8 -->intubate avoid decrease BP and decrease O2 secondary survey head to toe revaluation definitive care glasgow coma score post-traumatic subarachnoid a/w 39% motality causes severe post traumatic headache a/w underlying brain injury and cause major morbidity post-concussional syndrome behavioural change headaches dizziness irritable vertigo mood swings poor memory majority recover management neuropsychiatric assessment neuropsychimetric assessment - - Mindjet