
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Malignant skin cancer(cml)
Similar to Malignant skin cancer(cml) (20)
More from M Ridhwan Abd Razak
More from M Ridhwan Abd Razak (20)
Recently uploaded
Recently uploaded (20)
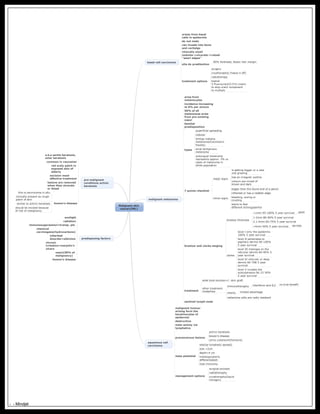
Malignant skin cancer(cml)
- 1. Malignant skin cancer(CML) basal cell carcinoma arises from basal cells in epidermis do not mets can invade into bone and cartialge clinically small nodules->ulcerate->raised ''pearl edges'' site do predilection 90% forehead, faceor hair margin treatment options surgery cryotheraphy( freeze it off) radiotherapy topical 5-fluorouracil(5-FU)-cream to stop uracil component to multiply malignant melanoma arise from melanocytes incidence increasing at 6% per annum 50% of all melanomas arise from pre existing naevi familial predisposition types superficial spreading nodular lentigo maligna melanoma(hutchison's freckle) acral lentiginous melanoma subungual melanoma represents approx. 3% oc cases of melanoma in white population 7 points checklist major signs is getting bigger or a new one growing has an irregular outline colours are mixed of brown and dark minor signs bigger than the blund end of a pencil inflamed or has a reddish edge bleeding, oozing or crusting starts to feel different-itching/painful breslow and clarke staging breslow thickness <1mm 95-100% 5 year survival good 1-2mm 80-96% 5 year survival 2.1-4mm 60-75% 5 year survival >4mm 50% 5 year survival terrible clarke level I only the epidermis 100% 5 year survival level II penetrates to papillary dermis 90-100% 5 year survival level III impinges on the reticular dermis 80-90% 5 year survival level IV reticular or deep dermis 60-70& 5 year survival level V invades the subcutaneous fat 15-30% 5 year survival treatment wide local excision+/- skin graft other treatment modalities immunotheraphy interferon and IL2 no true benefit chemo. limited advantage melanoma cells are radio resistant sentinel lymph node squamous cell carcinoma malignant tumour arising form the keratinocytes of epidermis destructive mets aminly via lymphatics precancerous lesions actinic keratosis bowen's disease cornu cutaneum(honours) mets potential site(lip-lymphatic spread) size >2cm depth>4 cm histology(poorly differentiated) host immunity management options surgical excision radiotheraphy cryotheraphy(liquid nitrogen) predisposing factors sunlight radiation immunosuppression=transp. pts chemical carcinogens(hydrocarbons) inherited disorder=albinism chronic irritation=marjolin's ulcers naevi(50% of malignancy) bowen's disease pre-malignant conditions actinic keratosis a.k.a senile keratosis, solar keratosis common in caucasian red scaly patch in exposed skin of elderly excision most effective treatment lesions are removed when they ulcerate or bleed bowen's disease this is carcninoma in situ clinically present as rough patch of skin similar to actinic keratosis should be excised because of risk of malignancy - - Mindjet