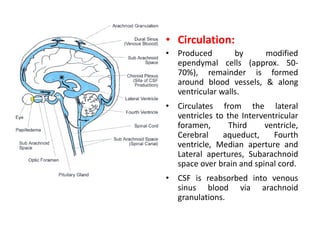
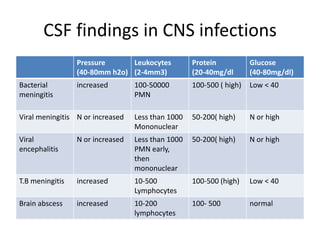
Lumbar puncture, or spinal tap, is indicated to check for meningitis, subarachnoid hemorrhage, or other central nervous system diseases. Contraindications include increased intracranial pressure, pending cerebral herniation, critical illness, skin infection at the site, or thrombocytopenia. Cranial CT is recommended before lumbar puncture for those with suspected meningitis or subarachnoid hemorrhage to check for masses or bleeding. Cerebrospinal fluid is produced and circulates through the brain and spinal cord before being reabsorbed into blood. Abnormal cerebrospinal fluid findings can indicate bacterial meningitis, viral meningitis, viral en


![Indications for performing brain CT
scanning before lumbar puncture
• in patients with suspected meningitis include the following[8] :
immunocompromised
with known CNS lesions
had a seizure within 1 week
abnormal level of consciousness
patients with focal findings on neurologic examination
papilledema &suspicion of an elevated ICP
• Cranial CT scanning should be obtained before lumbar puncture in
all patients with suspected SAH in order to diagnose obvious
intracranial bleeding or any significant intracranial mass effect that
might be present in awake and alert SAH patients with a normal
neurologic examination](https://image.slidesharecdn.com/csf-130527175809-phpapp01/85/Csf-4-320.jpg)