4. Causes of portal hypertensio
n
Pre hepati
c
• Congenital portal atresi
a
• Portal vein thrombosi
s
• Phlebitis of portal vei
n
Hepati
c
• Cirrhosi
s
• Chronic hepatiti
s
• Parasitic infections (schistosomiasis
)
Post hepati
c
• Budd-chiari syndrom ( Hepatic venus thrombosis
)
• Constructive pericarditi
s
• Tricuspid valve incompetence
6. Symptoms
Symptoms of portal hypertension include the following:
•
Weakness, tiredness, and malaise
•
Anorexia
•
Sudden and massive bleeding, with or without shock on
presentation
•
Nausea and vomiting
•
Weight loss
•
Abdominal discomfort and pain - Usually felt in the right
hypochondrium or under the right lower ribs (front, side, or back)
and in the epigastrium or the left hypochondrium
•
Jaundice
•
Edema and abdominal swelling
7. •
Pruritus
•
Spontaneous bleeding and easy bruising
•
Symptoms of encephalopathy
•
Impotence and sexual dysfunction
•
H e m a t e m e s i s o r m e l e n a - M a y i n d i c a t e
gastroesophageal variceal bleeding
•
Increasing abdominal girth - May indicate ascites
formation
•
Abdominal pain and fever - May indicate spontaneous
bacterial peritonitis
•
Hematochezia
8. Complications of portal hypertensio
n
ASCITES
• The mechanisms responsible for the development of ascites are
not completely understood. Portal hypertension and the resulting
increase in capillary pressure and obstruction of venous blood
fl
ow
through the damaged liver are contributing factors
.
• The failure of the liver to metabolize aldosterone increases sodium
and water retention by the kidney. Sodium and water retention,
increased intravascular
fl
uid volume, and decreased synthesis of
albumin by the damaged liver all contribute to
fl
uid moving from
the vascular system into the peritoneal space.
9. Pathophysiolog
y
Cirrhosis with portal hypertension
Splanchnic vasodilation
Decrease in circulating arterial blood volume
Activation of renin-angiotensin and sympathetic nervous systems and antidiuretic
hormone
Kidney retains sodium and water
Hypervolemia
Persistent activation of systems for retention of sodium and water; ascites and edema
formation
Continued arterial under
fi
lling; cycle repeats
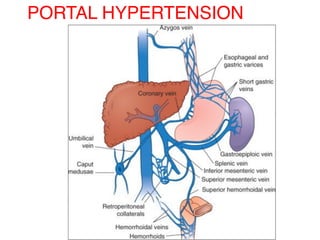
10. Clinical Manifestations
• Increased abdominal girt
h
• Rapid weight gai
n
• S h o r t o f b r e a t h a n d
uncomfortable from the
enlarged abdome
n
• Striae and distended veins may
be visible over the abdominal
wall (caput medusa).
• Umbilical hernia
• F l u i d a n d e l e c t r o l y t e
imbalances are common.
11. ESOPHAGEAL VARICES
Esophageal varices are dilated veins usually
found in the submucosa of the lower
esophagus, but they may develop higher in
the esophagus or extend into the stomach.
This condition nearly always is caused by
portal hypertension, which in turn is due to
obstruction of the portal venous circulation
within the damaged liver.
12. Risk factor
s
Risk factors that contribute to hemorrhage
are;
•Muscular exertion from lifting heavy
object
s
•Straining at stoo
l
•Sneezing, coughing, or vomitin
g
•Esophagitis; irritation of vessels by poorly
chewed foods or irritating
fl
uids; or re
fl
ux
of stomach contents.
13. Pathophysiology
Portal hypertension
Development of pressure gradient of 12 mm Hg or greater
Venous collaterals develop
from high portal system pressure to systemic vein
s
Formation of abnormal varicoid vessel
s
Vessels may rupture causing life-threatening hemorrhage.
16. Medical Management
DIETARY MODIFICATION
The goal of treatment for the patient with
ascites is a negative sodium balance to
reduce
fl
uid retention
.
DIURETICS
Use of diuretics along with sodium
restriction is successful in 90% of patients
with ascites.
PARACENTESIS
Paracentesis is the removal of
fl
uid (ascites)
from the peritoneal cavity through a small
surgical incision or puncture made through
the abdominal wall under sterile conditions.
17. Beta-blocker
s
Beta-blockers (nadolol or propranolol) may be
prescribed to reduce the pressure in varices and further
reduce the risk of bleeding
.
BALLOON TAMPONADE
To control hemorrhage in certain patients, balloon
tamponade may be used. In this procedure, pressure is
exerted on the cardia (upper ori
fi
ce of the stomach) and
against the bleeding varices by a balloon tamponade.
The tube has four openings, each with a speci
fi
c
purpose: gastric aspiration, esophageal aspiration,
in
fl
ation of the gastric balloon, and in
fl
ation of the
esophageal balloon.
18.
19. ENDOSCOPIC SCLEROTHERAPY
In endoscopic sclerotherapy (also referred to as injection
sclerotherapy), a sclerosing agent is injected through a
fi
beroptic
endoscope into the bleeding esophageal varices to promote thrombosis
and eventual sclerosis.
20. ESOPHAGEAL BANDING THERAPY (VARICEAL BAND LIGATION)
In variceal banding, a modi
fi
ed endoscope loaded with an elastic rubber
band is passed through an over-tube directly onto the varix (or varices) to be
banded. After suctioning the bleeding varix into the tip of the endoscope, the
rubber band is slipped over the tissue, causing necrosis, ulceration, and
eventual sloughing of the varix.
21. TRANSJUGULAR INTRAHEPATIC PORTOSYSTEMIC
SHUNTING
Transjugular intrahepatic portosystemic shunting (TIPS) is a method of
treating esophageal varices in which a cannula is threaded into the
portal vein by the transjugular route. An expandable stent is inserted
and serves as an intrahepatic shunt between the portal circulation and
the hepatic vein, reducing portal hypertension.
22. SURGICAL MANAGEMENT
Several surgical procedures have
b e e n d e v e l o p e d t o t r e a t
esophageal varices and to
minimize rebleeding, but they are
often accompanied by signi
fi
cant
risk. Procedures that may be used
for esophageal varices are;
splenorenal and portacaval
venous shunts to relieve portal
pressure.