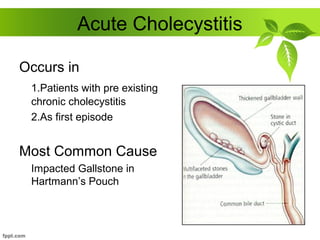
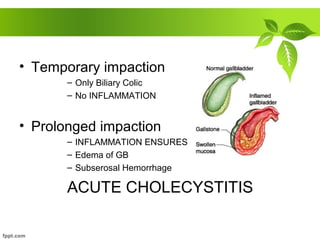
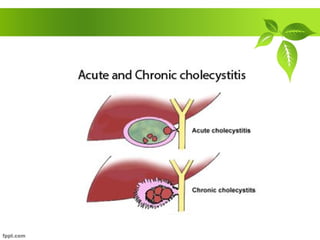
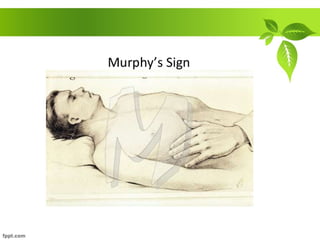
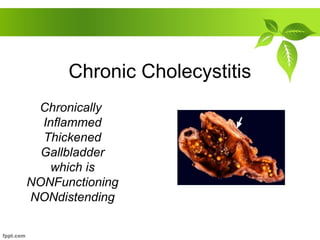
This document discusses acute and chronic cholecystitis. Acute cholecystitis typically occurs due to gallstone impaction and results in inflammation of the gallbladder. Common symptoms include fever, right upper quadrant pain, and nausea. Diagnosis involves physical exam findings like Murphy's sign along with supportive lab and ultrasound results showing gallstones, thickened gallbladder walls, and pericholecystic fluid. Treatment involves antibiotics, pain medication, and cholecystectomy usually within 3 days. Chronic cholecystitis is due to long-standing gallstones or cholecystoses and results in a thickened, non-functioning gallbladder. Cholecystectomy is the treatment for chronic cholecystitis.

































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)








