Downloaded 1,857 times
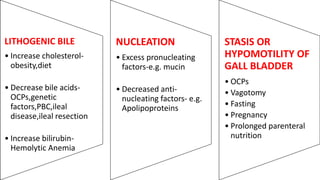
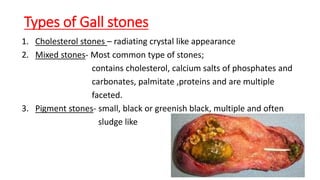
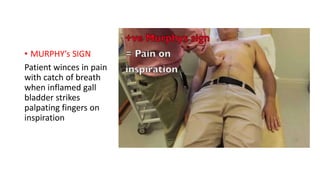


This document discusses predisposing factors, pathogenesis, types, clinical features, complications, investigations, differential diagnosis, and management of gallstones. The main types are cholesterol stones, mixed stones, and pigment stones. Risk factors include obesity, female sex hormones, age, pregnancy, certain drugs, and diabetes. Gallstones can cause symptoms like biliary colic or be asymptomatic. Complications involve inflammation of the gallbladder or bile ducts. Treatment options are medical therapy with ursodeoxycholic acid for small cholesterol stones or laparoscopic cholecystectomy.








































































![Cells and Organs of immune system [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/cellsandorgansofimmunesystemautosaved-260123152717-ea0cb261-thumbnail.jpg?width=640&height=640&fit=bounds)





