Downloaded 185 times



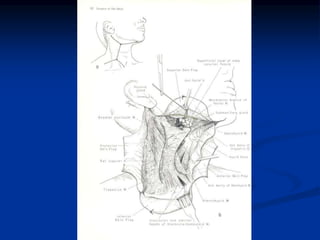
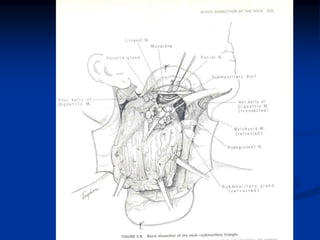
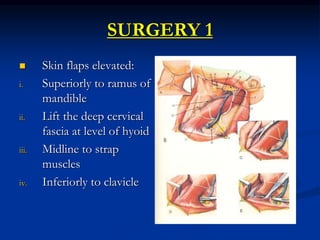
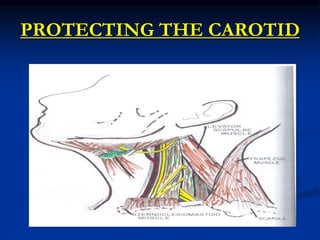
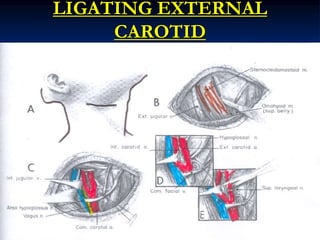

Elevate the skin flaps superiorly to the level of the ramus of mandible. Identify and protect the external jugular vein. Surgeon: Okay, elevating the skin flaps now. Carefully dissecting in the plane just deep to the platysma muscle. There's the external jugular vein, I'm protecting that as I elevate the flap. Almost to the level of the ramus now.








































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)









![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)




