Download as PDF, PPTX







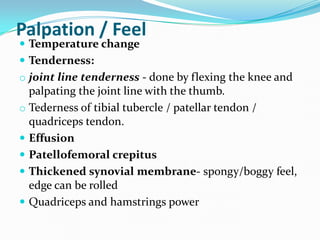
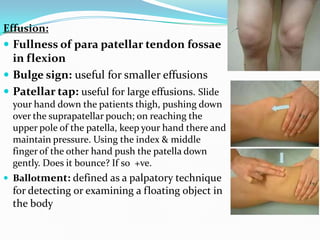
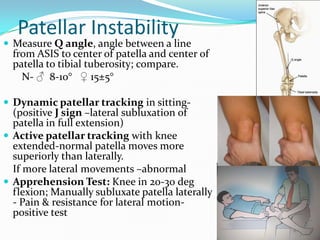

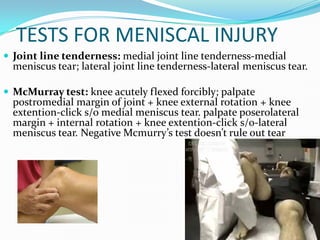
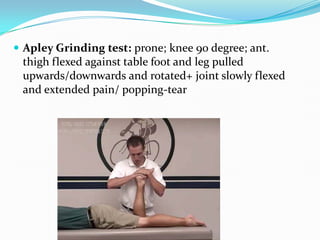

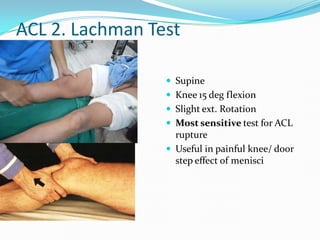
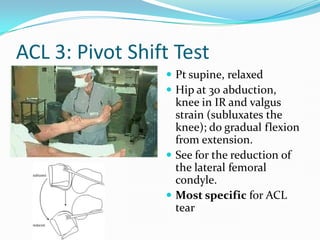




The document summarizes the process for examining the knee, including: - Inspecting for alignment, masses, scars while standing or supine - Palpating for temperature, tenderness, effusion, crepitus, strength - Testing range of motion including flexion, extension, rotation - Performing tests like McMurray's, Lachman, and valgus/varus stress to check for injuries to structures like the meniscus, ACL, MCL, and LCL




























































