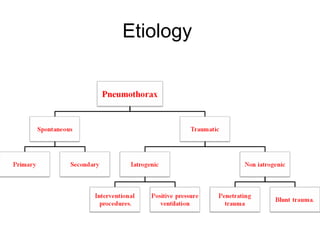
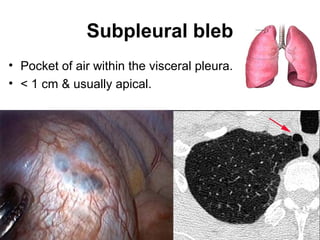
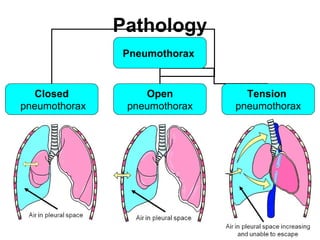
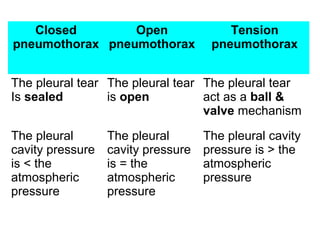
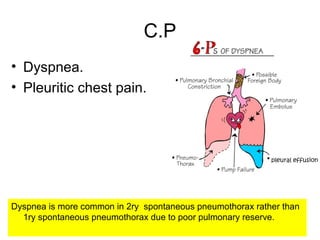
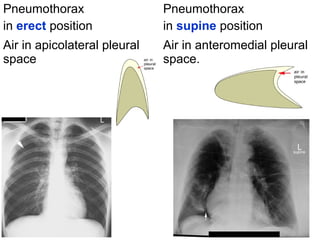
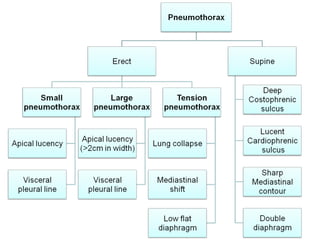
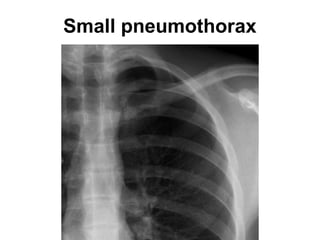
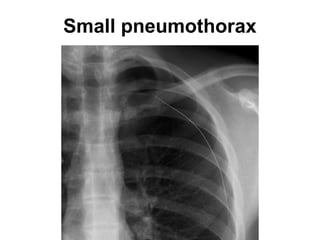
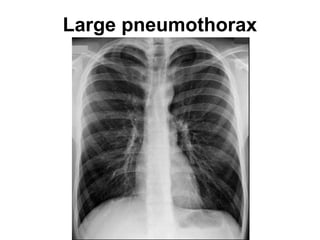
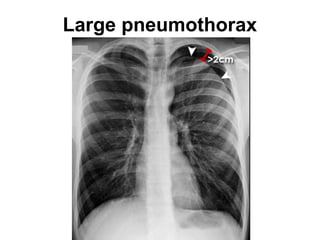
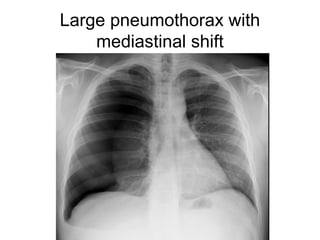
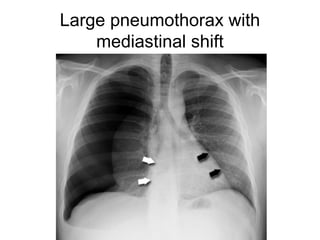
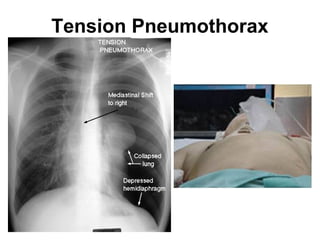
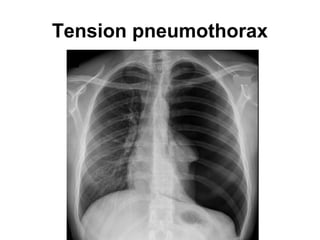
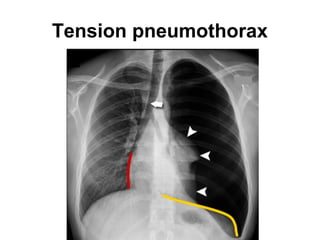
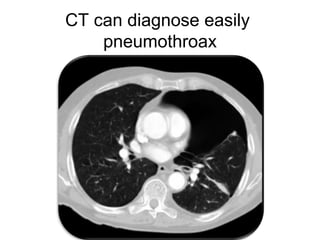
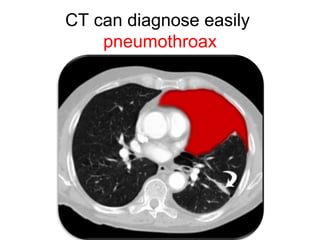
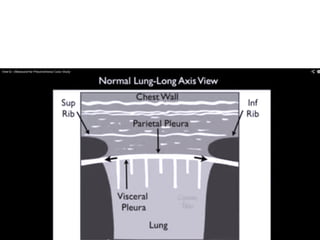
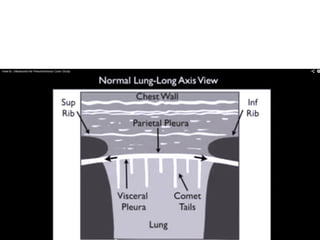
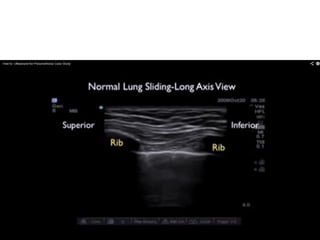
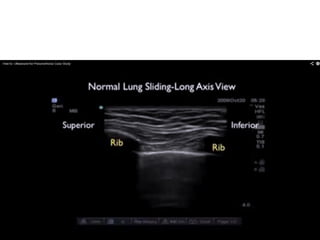
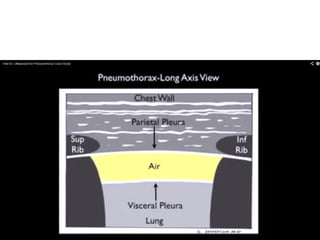
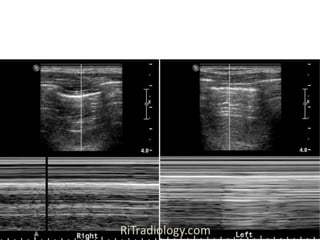
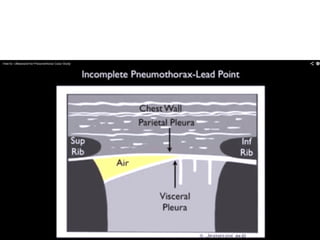
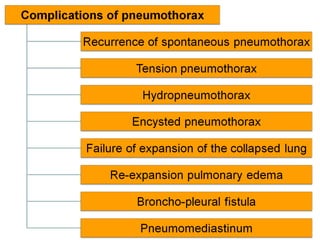
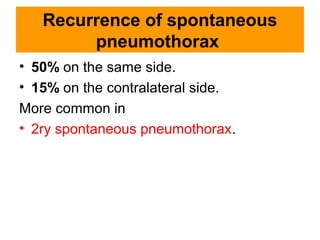
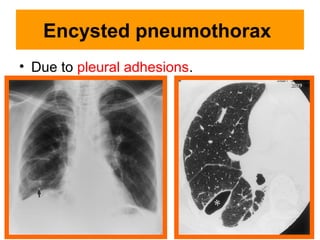
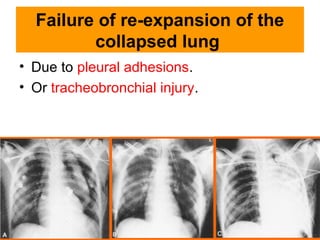
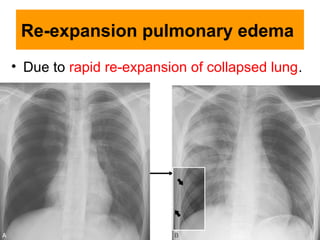
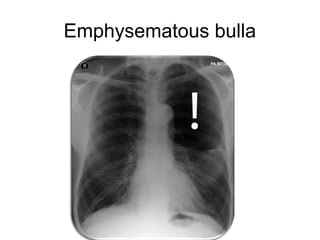
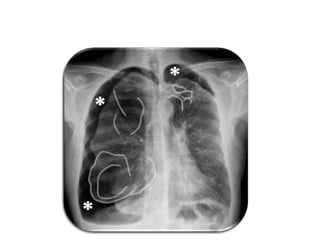
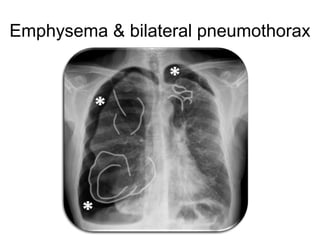
This document discusses pneumothorax, beginning with the causes and types. Primary spontaneous pneumothorax is usually caused by a ruptured bleb and occurs more often in young, thin males who smoke. Secondary spontaneous pneumothorax has an underlying lung disease like emphysema. Traumatic pneumothorax results from blunt or penetrating chest trauma or medical procedures. Imaging findings and complications are also described, including recurrent pneumothorax, tension pneumothorax, and re-expansion pulmonary edema. Ultrasound is a sensitive test for pneumothorax diagnosis.









































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)







