2. DEFINITION
Osteitis: a general term for inflammation of
the bone
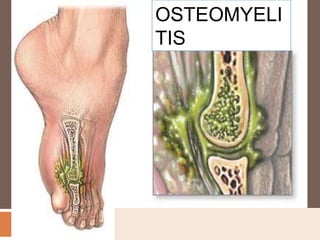
Osteomyelitis is a severe pyogenic infection
and inflammation of bone and surrounding
tissues
3. CLASSIFICATION
Based on mode of entry – classified in to
Exogenous osteomyelitis
Endogenous or hematogenous osteomyelitis
Based on the duration
Acute and chronic ostoemyelitis
4. Exogenous osteomyelitis
Onset is insidious
Infection begins in soft tissues, disrupting muscle
and connective tissue and eventually forming
abscess
Caused by a pathogen outside the body or by the
spread of infection from adjacent soft tissues.
Example – from an open fracture or a surgical
procedure, can also caused by human and animal
bites
The infection spreads from soft tissues to the bone
5.
6. Hematogenous osteomyelitis
Caused by blood borne pathogens originating
from infectious sites within the body
Example –from sinus, ear, dental, respiratory
and genitourinary infections
In this the infection spreads from the bone to
the soft tissues and eventually break through
the skin becoming draining fistula
More common in children's and older adults
7.
8. RISK FACTORS
Soft tissue infections and direct bone
contamination (surgery, gunshot)
Chronic illness
Diabetes or vascular disease
Alcohol or drug abuse
Immunosuppression
Elderly
Poorly nourished
Obese patients
9. ETIOLOGY
Bacteria
Viruses
Fungi and parasites
Common microorganisms are S.aureus,
streptococcus, hemophilus influenzae
enterobacteria, salmonella
Entry of organism from an open wound or
hematogenous spread
10. PATHOPHYSIOLOGY
In hematogenous osteomyelitis
Organisms reach the bone through the circulatory
and lymphatic systems
Bacteria lodge in the small vessels of the bone
Inflammation
Blockage of the vessel causes thrombosis, ischemia
and necrosis of bone
(femur, tibia, humerus and radius are commonly
11. Bacteria and inflammation spread within the shaft of the
bone and spread throughout the haversian systems
and reach the periosteum
Subperiosteal abscess
Segmental bone necrosis sequestrum (dead piece of
bone)
new bone laid down over the infected bone by
osteoblasts is called as involucrum- opening in the
involucrum allow infected material to escape into soft
tissue
12. CLINICAL FEATURES
Acute osteomyelitis – less than one month in
duration
CM of acute osteomyelitis are both systemic and
local
Systemic – fever, night sweats, chills,
restlessness, nausea and malaise
Local – severe bone pain unrelieved by rest and
worse with activity, swelling, tenderness, warmth
at the site
Later signs include drainage from sinus tracts to
the skin and fracture site
15. DIAGNOSTIC EVALUATION
History collection
Physical examination
Lab studies - elevated WBC, c-reactive protein (CRP)
and erythrocyte sedimentation rate (ESR)
BLOOD CULTURE – to find out the organisms
CT scan and radionuclide bone scan
X ray ,MRI, Bone biopsy
17. SURGICAL MANAGEMENT
Debridement surgery
To remove necrotic tissue
Removal of sequestrum and surrounding
granulation tissue (sequestrectomy)
The dead space is later filled with, antibiotic
beads (polymethylmethacrylate beads with either
vancomycin, tobramysin or gentamicin),tissue
flaps and bone grafts
Beads are usually removed after 2 to 4 weeks and
reconstruction is performed
18.
19.
20.
21. Osteomyelitis with fracture
Bone graft and internal or external fixation
together
Ilizarov technique – helps in bone lengthening
and reshaping.
Papineau technique - type of open bone
grafting technique in which wounds are
packed with cancellous bone with no attempt at
soft tissue coverage.
22.
23.
24. COMPLICATIONS
Sepsis
Pathologic fracture and non
union
Draining fistula
Shortening of the extremity
Amputation
Brodie’s abscesses –
isolated encapsulated
pockets of microorganisms
surrounded by bone matrix –
capable of reinfection at any
25. MEDICAL MANAGEMENT
Antipyretics and analgesics
Antibiotic therapy – penicillin, cephalosporin,
Clindamycin
Depends on the causative organism
2 to 4 weeks IV followed by 4 weeks oral
medication
3 to 6 weeks in case of orthopedic implants
Hyperbaric oxygen therapy may be used
26. NURSING MANAGEMENT
Maintain aseptic technique during dressing
Observes for signs and symptoms of
complications
Timely medication – for effective action of
antibiotics
Complete rest for early healing
Fracture prevention
Use splints and other assistive devices
ROM exercises to prevent contractures and
functional deformities
Provide diet high in vitamins and proteins
28. Relieving pain
Restrict activity
Immobilize affected part – use splints
Handle affected part with care
Elevate affected part to reduce swelling and
discomfort
Administer prescribed analgesic
Monitor neurovascular status of affected
extremity
29. Controlling infectious process
Monitor response of treatment
Observe IV sites for phlebitis or infiltration
If surgery is planned, ensure adequate
circulation
Maintain aseptic technique
Avoid pressure on grafted area
Monitor general health
Provide a balanced diet high in protein and
vitamin C to promote healing
30. Home and community based
care
Self care
Strict therapeutic regimen of antibiotics
Prevention of falls
Teach patient how to maintain and manage the IV
access site and equipment it there
Provide medical education (drug name, dose,
frequency and administration)
Instruct patient to observe for elevated temp, drainage,
adverse reactions
Teach patient and family how to perform aseptic
dressing
Explain the importance of follow up