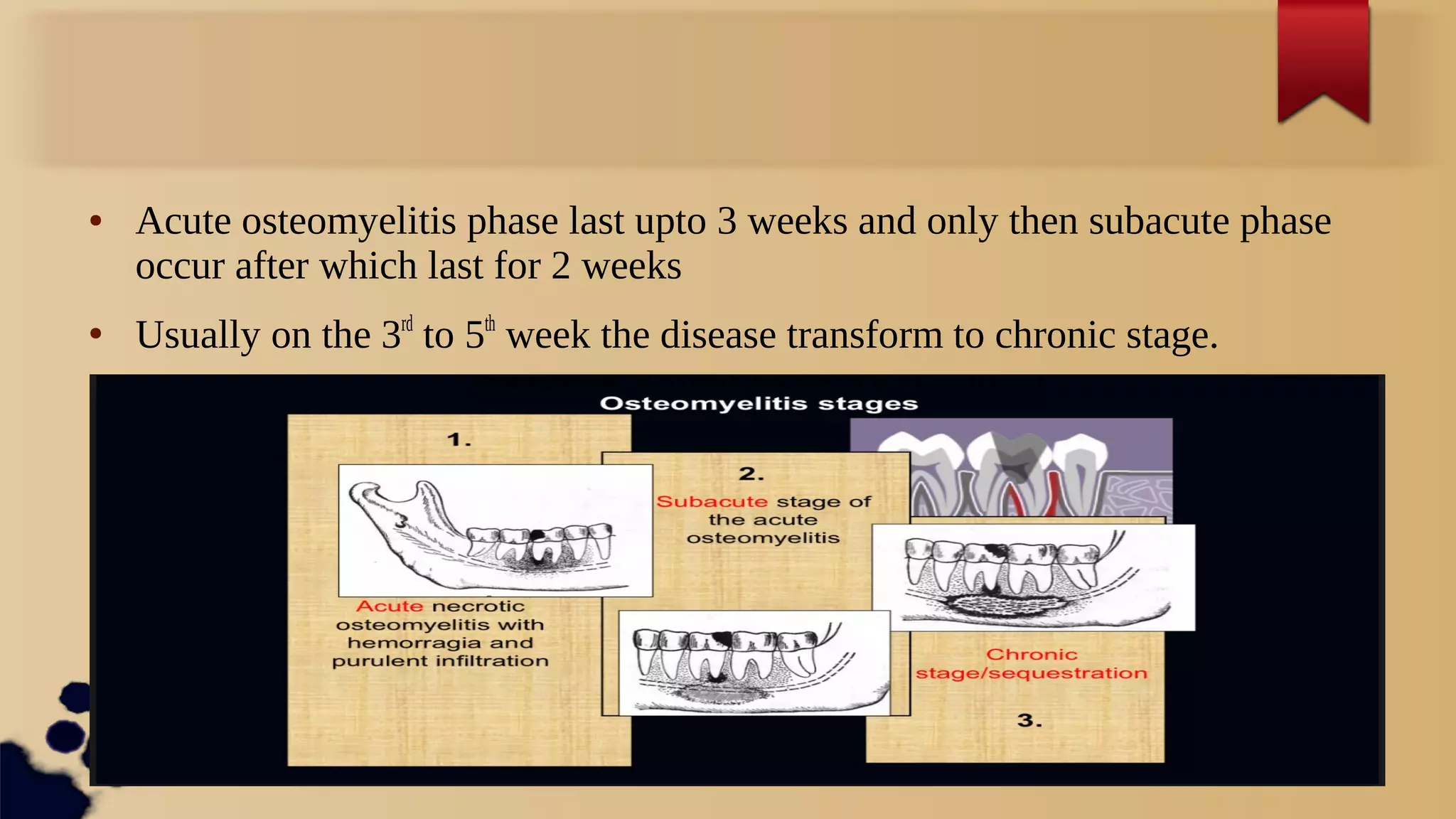
Download as ODP, PPTX














This document summarizes different types and stages of chronic osteomyelitis. It begins by defining subacute and chronic osteomyelitis, noting that the disease typically transitions from acute to chronic between 3-5 weeks. It then describes key features of different chronic forms, including hyperplastic (thickened bone), sequestering (decreased blood flow causes bone necrosis), and rarefying (diffuse process with small sequesters). The treatment section outlines extracting causative teeth, long-term antibiotic therapy, antifungal therapy to prevent dysbacteriosis, and surgical procedures like sequesterectomy to remove bone fragments. It concludes by differentiating osteomyelitis from related conditions like apical periodontitis and peri



































































