Tissue engineering
•Download as PPTX, PDF•
15 likes•2,753 views

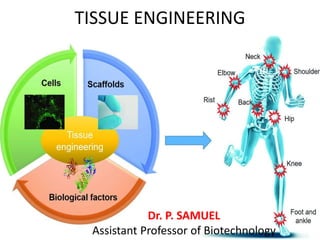
Tissue engineering components of tissue engineering Stem cell applications

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Tissue engineering
Similar to Tissue engineering (20)
More from AYYA NADAR JANAKI AMMAL COLLEGE
More from AYYA NADAR JANAKI AMMAL COLLEGE (17)
Recently uploaded
Recently uploaded (20)
Tissue engineering
- 1. TISSUE ENGINEERING Dr. P. SAMUEL Assistant Professor of Biotechnology
- 2. Introduction • Tissue Engineering is an interdisciplinary discipline addressed to create functional three-dimensional (3D) tissues combining scaffolds, cells and/or bioactive molecules. • The term Tissue Engineering (TE) was first presented to the broad scientific community in 1993 by Langer and Vacanti . • TE is the development of biological substitutes that maintain, improve or restore tissue function. • TE could sidestep the problems associated with tissue damage, in the present treated with transplants, mechanical devices or surgical reconstruction.
- 3. • These three medical therapies have saved and improved countless patients’ lives, but they present associated problems. • For example, organ transplants show important limitations such as transplant rejection and lack of donor to cover all the worldwide demand. • Mechanical devices are not capable of accomplishing all the functions associated with the tissue and cannot prevent progressive patient deterioration. • Finally, surgical reconstruction can result in long-term problems. • Therefore, TE arises from the need to provide more definitive solutions to tissue repair in clinics and aims to achieve this goal by the development of in vitro devices that would repair in vivo the damaged tissue.
- 4. • TE also leads to engineered tissues, which could allow us to study human physiology in vitro. • Cells in the body grow within an organized 3D Extra-Cellular Matrix (ECM), surrounded by other cells. • Indeed, the interactions between cell-cell and cell-ECM can determine whether a given cell undergoes proliferation, differentiation, apoptosis or invasion. • However, studies on cellular biology have commonly been performed on 2D cultures, where cells grown under non- physiological conditions. • Specifically, they are unnaturally polarized having one side attached to a rigid and flat substrate and the other one exposed to culture media, which reduces cell-cell and cell-ECM interactions.
- 5. Scaffold A major goal in TE is the design of scaffolds capable of recreating the in vivo microenvironment, which is mainly provided by the ECM. Regarding biophysical signaling, an essential function of the ECM is to give anchorage to cells. Indeed, the ECM highly porous nanostructure provides them a proper 3D microenvironment and imparts biochemical signaling through two mechanisms: (i) the binding of a wide variety of soluble Growth Factors (GF), enzymes and other effector molecules, controlling their diffusion and local concentrations and (ii) the exposure of specific motifs that are recognized by cellular adhesion receptors.
- 6. Properties of Biomaterials •An ideal biomaterial designed for clinical applications should fulfill a serial of requirements. •First of all, biocompatibility and biodegradability are required; allowing scaffold replacement by proteins synthesized and secreted by native or implanted cells. •Besides, the material must be clinically compliant (Good Manufacturing Practice) to minimize inflammatory and immunological response avoiding further tissue damage. •Moreover, as cell degradation products are toxic to other cells, it would be important that the material allow host macrophages to infiltrate and remove cellular debris. •Finally, material production, purification and processing should be easy and scalable.
- 7. •Scaffolds for TE can be divided in natural and synthetic, depending on its origin. • Natural scaffolds are readily accessible and provide a broad range of cues that in vivo participate in the process of morphogenesis and function acquisition of different cell types. •However, its composition strongly depends on the specific animal origin and the isolation and purification procedures, compromising assay reproducibility. •On the other hand, synthetic scaffolds can be custom tailored to mimic specific ECM properties, providing controllable cellular environments. Polymeric Scaffolds for Tissue Engineering
- 8. What are biomaterials? Biomaterials play an integral role in medicine today—restoring function and facilitating healing for people after injury or disease. The first historical use of biomaterials dates to antiquity, when ancient Egyptians used sutures made from animal sinew. The modern field of biomaterials combines medicine, biology, physics, and chemistry, and more recent influences from tissue engineering and materials science. Metals, ceramics, plastic, glass, and even living cells and tissue all can be used in creating a biomaterial. They can be reengineered into molded or machined parts, coatings, fibers, films, foams, and fabrics for use in biomedical products and devices. These may include heart valves, hip joint replacements, dental implants, or contact lenses. They often are biodegradable, and some are bio-absorbable, meaning they are eliminated gradually from the body after fulfilling a function.
- 9. • Hydrogel sealants may allow pain-free dressing changes for patients with burns. • Grinstaff lab, Boston University
- 10. How are biomaterials used in current medical practice? Doctors, researchers, and bioengineers use biomaterials for the following broad range of applications: Medical implants, including heart valves, stents, and grafts; artificial joints, ligaments, and tendons; hearing loss implants; dental implants; and devices that stimulate nerves. Methods to promote healing of human tissues, including sutures, clips, and staples for wound closure, and dissolvable dressings. Regenerated human tissues, using a combination of biomaterial supports or scaffolds, cells, and bioactive molecules. Examples include a bone regenerating hydrogel and a lab-grown human bladder. Molecular probes and nanoparticles that break through biological barriers and aid in cancer imaging and therapy at the molecular level. Biosensors to detect the presence and amount of specific substances and to transmit that data. Examples are blood glucose monitoring devices and brain activity sensors. Drug-delivery systems that carry and/or apply drugs to a disease target. Examples include drug-coated vascular stents and implantable chemotherapy wafers for cancer patients.
- 11. Cells An important decision to make when designing strategies for TE is the cell source selection. This step becomes a critical issue especially when these strategies are designed to be clinically applied. Importantly, cells should fulfill a basic requirement: integrate themselves in the specific tissue and secret various GF and cytokines that activate the endogenous tissue regeneration program. The first approach in cell based techniques is the use of native progenitor cells. The main problem is the inherent difficulty of growing some specific cell types to obtain large quantities. As a consequence, stem cells either Embryonic (ESCs) or Adult (ASCs) have emerged as promising alternative cell sources. An alternative cell type under study for their application in TE are induced Pluripotent Stem Cells (iPSCs), which were first generated by Yamanaka and collaborators.
- 12. Biomolecules Besides an appropriate scaffold and cell source, signaling molecules represent an interesting tool in TE to modulate several aspects of cell biology, from proliferation capacity to specific phenotypic features of fully differentiated cells. In the cellular environment, the presence and gradient of soluble factors such as GF, chemokines, and cytokines play an important role in biological phenomena such as chemotaxis, morphogenesis and wound healing. In particular, these signals are tightly controlled and unique to each organ. Signaling molecules used in TE can be added to the culture media as soluble factors or attached to the scaffold by covalent and non-covalent interactions. Consequently, the controlled release of different factors from scaffolds allows their constant renewal, having a great potential to direct tissue regeneration and formation. Several matrix systems, micro particles and encapsulated cells have been reported to locally deliver bioactive factors and to maintain effective concentrations for their use in the application areas, such as musculoskeletal, neural and hepatic tissue.
- 13. Applications of stem cell Stem cells from the umbilical cord are special. They are young, potent, and viable. Numerous clinical studies are being conducted worldwide researching the suitability of stem cells for the regeneration of damaged tissues after accidents, degenerative diseases like e.g. slipped intervertebral discs, or cancer treatment. Many health professionals and scientists believe in the potential of stem cells: Umbilical cord blood and tissue that is rich in stem cells will be an important therapeutic option in future medicine.
- 15. Stem cell in cancer therapy • Stem cells have been applied in the treatment of serious diseases for more than 55 years. • They are applied especially to treat cancers, which require high- dose chemotherapy within the scope of medical care. • The patient’s own stem cells are extracted from bone marrow or peripheral blood prior to high- dose chemotherapy, stored temporarily and transplanted after the treatment in order to minimize the side effects of the aggressive chemotherapy and to support the regeneration of destroyed cells.
- 16. Besides cancer, several 100,000 people come down with common diseases like dementia, which belongs to the neurodegenerative diseases, cardiac infarction, stroke, arthritis, or diabetes every year. The lifelong therapy causes enormous costs in the health care system. Stem cell therapy offers great potential for the treatment of such diseases. Experts expect that every seventh person up to the age of 70 will need a therapy based on stem cells in the future to regenerate sick or aged cells and tissues.
- 17. The possible applications of stem cells increase
- 18. Stem cells have already been applied successfully for: Hematopoietic disorders Acute and chronic leukemia (AML/ALL or CML/CLL) Myelodysplastic syndrome Lymphomas (Hodgkin lymphoma, non-Hodgkin lymphoma) Aplastic anemia Sickle cell anemia Beta thalassemia Immunodeficiency SCID Whiskott Aldrich syndrome Metabolic disorders Mucopolysaccharidosis Cancer Multiple myeloma Neuroblastoma
- 20. Stem cell therapy is a promising option for repairing heart tissue damaged by heart attack. However, the main obstacle to cardiac stem cell therapy also happens to be pretty difficult to get around – and that's the fact that the heart is constantly in motion. "Cell retention is always problematic when you do cell transplantation, but in the heart it is particularly difficult," says Ke Cheng, associate professor of regenerative medicine at NC State. "The heart's pumping can wash cells out of the organ and they'll either disappear or end up in other organs – where they are essentially wasted. “Cheng specializes in regenerative medicine, and he wanted to address the problem of keeping cardiac stem cells where they belong long enough for them to settle in and start working. In 2010, he showed that it was possible to attach an iron nanoparticle to cardiac stem cells and use a magnetic field to keep the cells where they needed to be.
- 21. Now, Cheng has taken his process one step further. In a recently published paper in Biomaterials, Cheng used nanoparticles from an FDA-approved anemia drug called Feraheme to label the cardiac stem cells, then used magnets to direct the cells to the hearts of rats with cardiac disease. "The magnetic field dramatically improved cell retention and the therapeutic effects," Cheng says. "We're talking about a three-fold increase in cell retention. And the fact that the label we used is an already FDA-approved drug means that we are one step closer to bringing the therapy to clinical trials in humans."
- 22. Stem cell self renewal mechanism • Self-renewal is the process by which stem cells divide to make more stem cells, perpetuating the stem cell number throughout life. • Self-renewal is division with maintenance of the undifferentiated state. • This requires cell cycle control and often maintenance of multipotency or pluripotency, depending on the stem cell. • Self-renewal programs involve networks that balance proto-oncogenes (promoting self-renewal), gate-keeping tumor suppressors (limiting self-renewal), and care- taking tumor suppressors (maintaining genomic integrity). • These cell-intrinsic mechanisms are regulated by cell-extrinsic signals from the niche, the microenvironment that maintains stem cells and regulates their function in tissues. • In response to changing tissue demands, stem cells undergo changes in cell cycle status and developmental potential over time, requiring different self-renewal programs at different stages of life. Reduced stem cell function and tissue regenerative capacity during aging are caused by changes in self-renewal programs that augment tumor suppression. Cancer arises from mutations that inappropriately activate self-renewal programs.
- 23. THE REGULATION OF PLURIPOTENT STEM CELL SELF-RENEWAL • Embryonic stem (ES) cells are derived from the inner cell mass of the blastocyst prior to implantation. • They possess indefinite self-renewal potential as well as the ability to generate all cell types within the body (pluripotency). • These characteristics distinguish ES cells from tissue stem cells, which have more limited self renewal and developmental potentials. • The unlimited self-renewal potential and pluripotency of ES cells are conferred by unique transcriptional and cell cycle regulation (Jaenisch & Young 2008).