- The patient presented with an acute ankle fracture dislocation of the left ankle secondary to a motor vehicle accident. Imaging showed a displaced fracture of the medial and lateral malleolus.
- The plan is to perform a closed or open reduction with multiple pinning of the lateral and medial malleolus of the left ankle as an urgent case. Laboratory results were notable for elevated inflammatory markers.
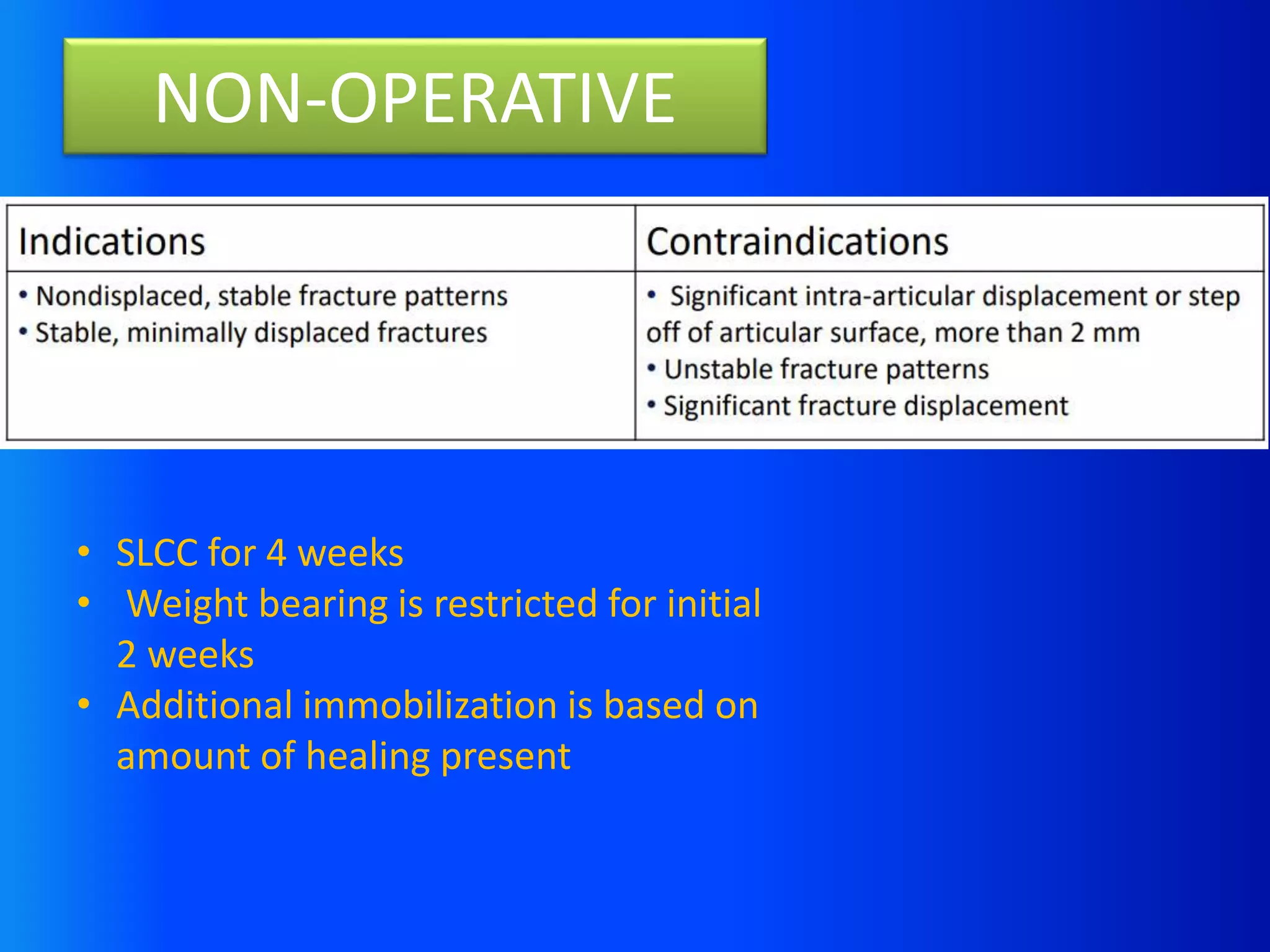
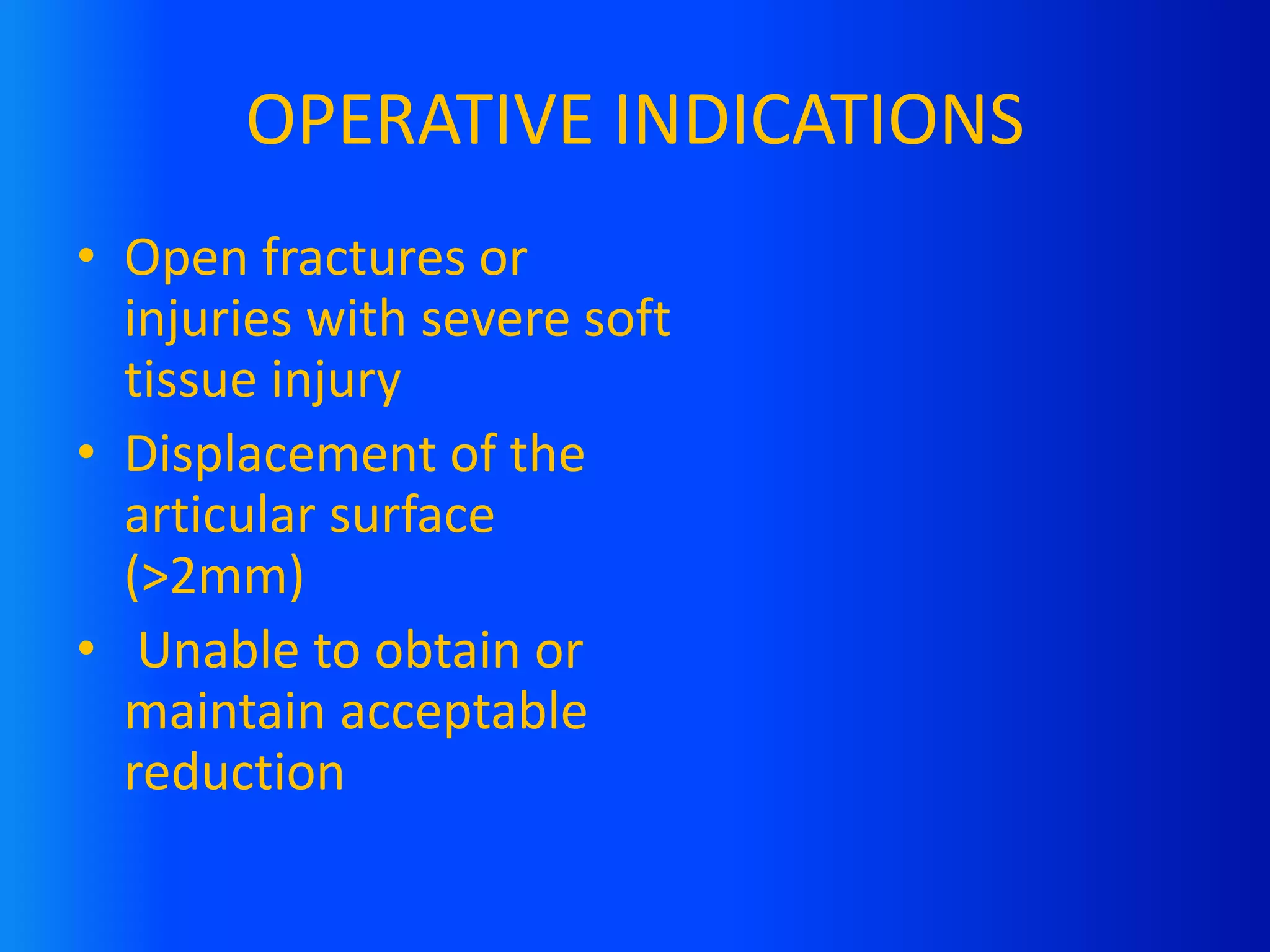
- Key ankle anatomy and the classification of pediatric ankle fractures are discussed to guide treatment, which may involve non-operative management with casting or operative intervention with pinning depending on the fracture pattern and displacement.