Downloaded 36 times

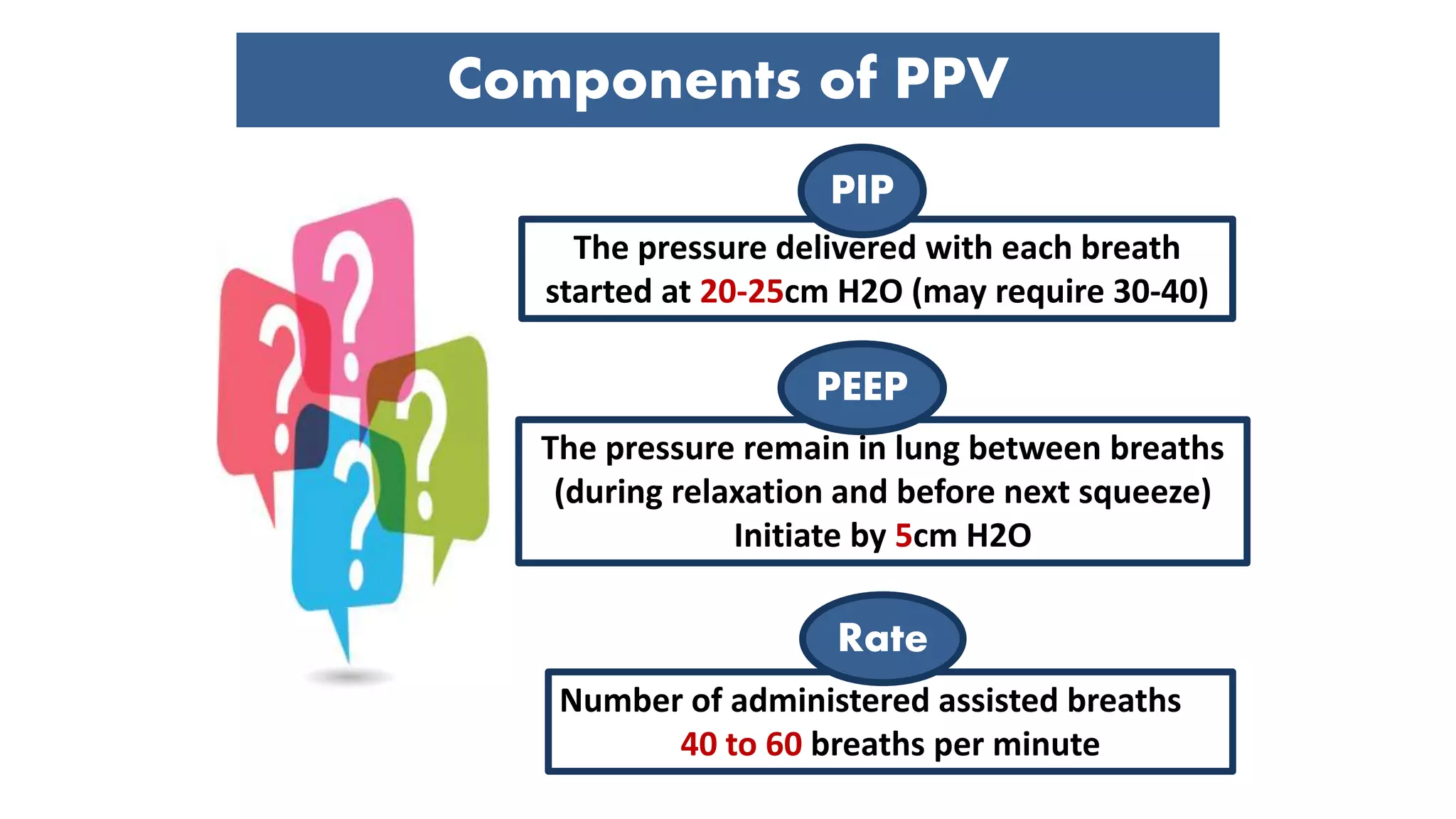
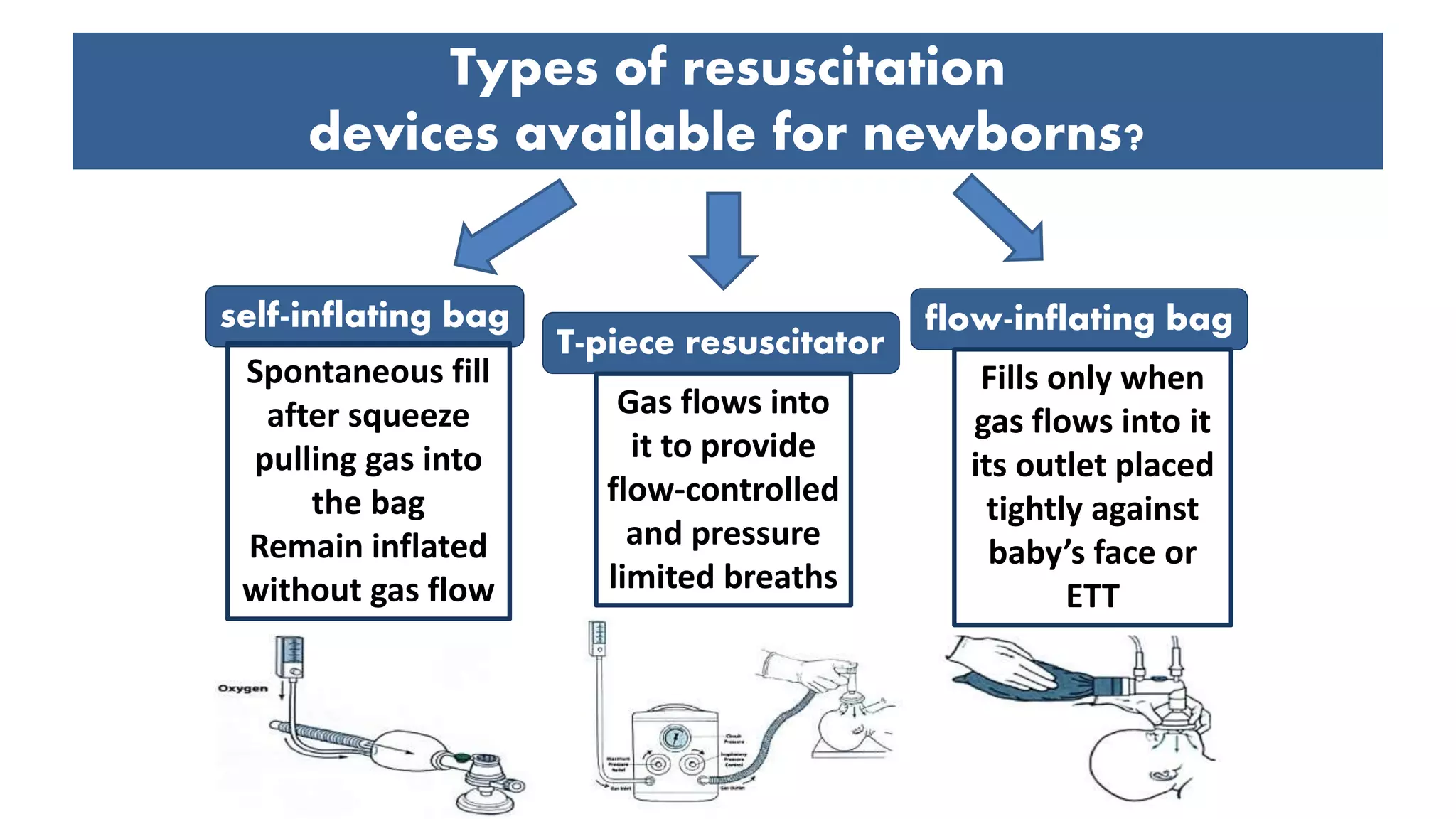
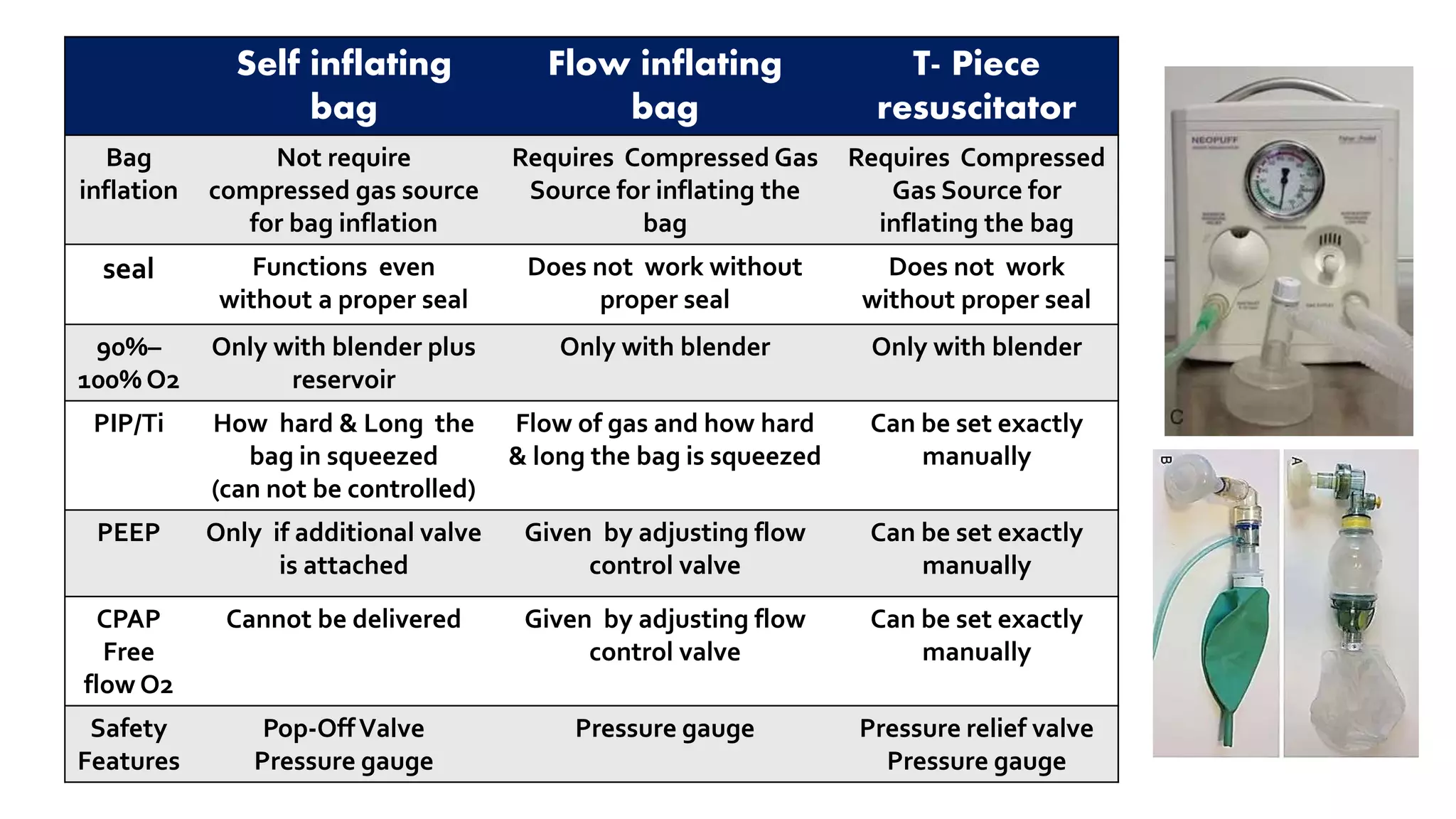
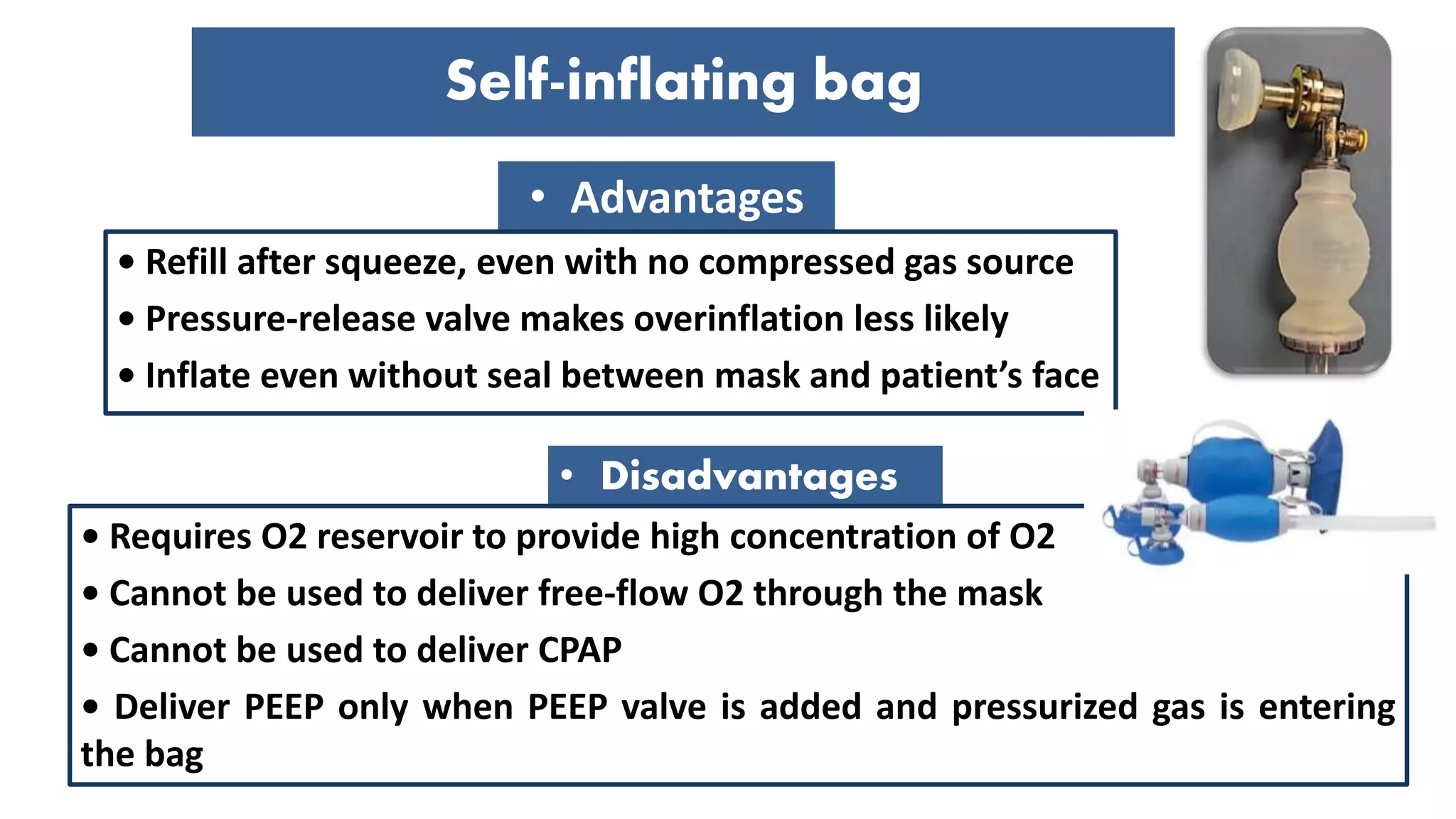
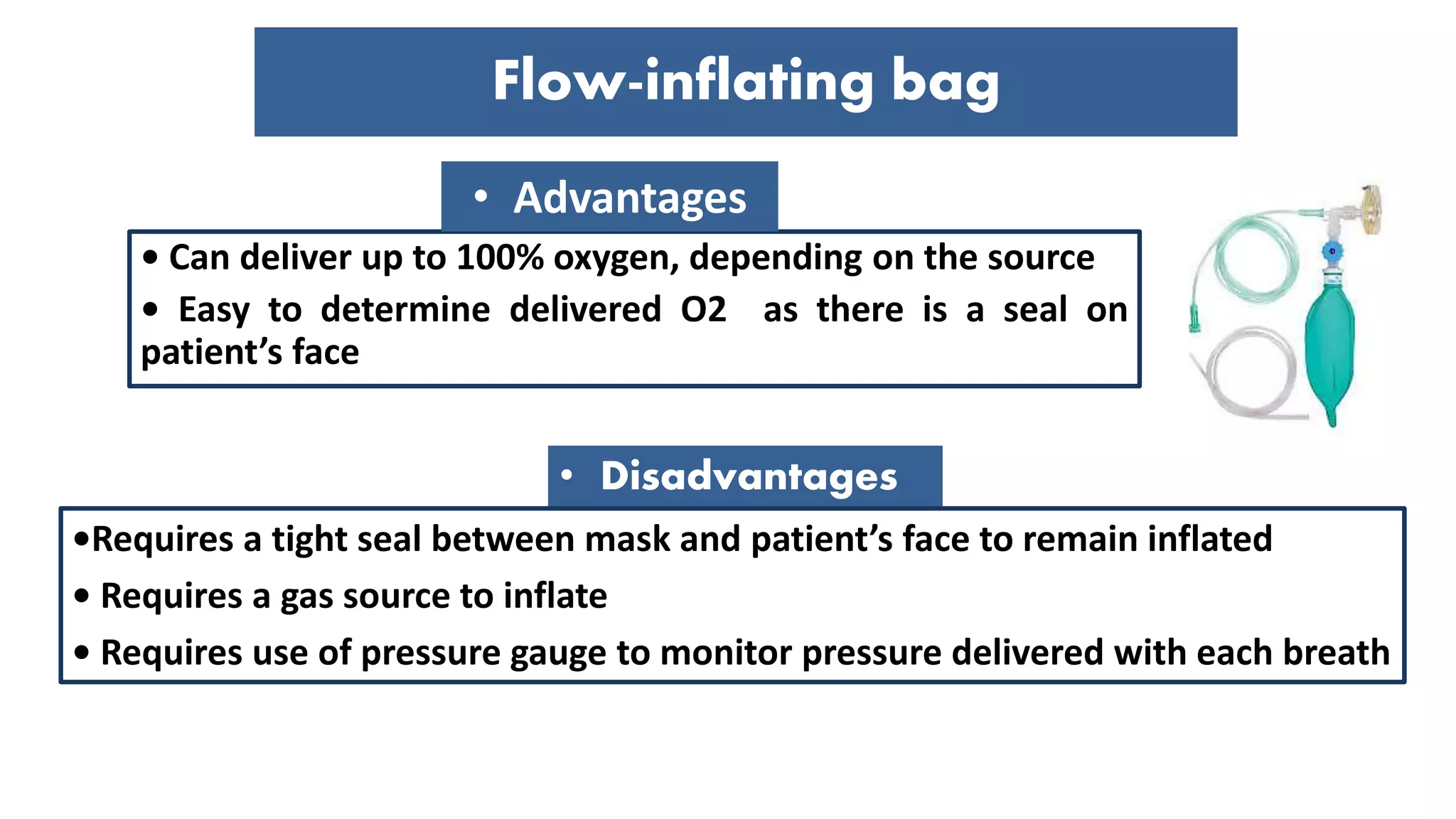
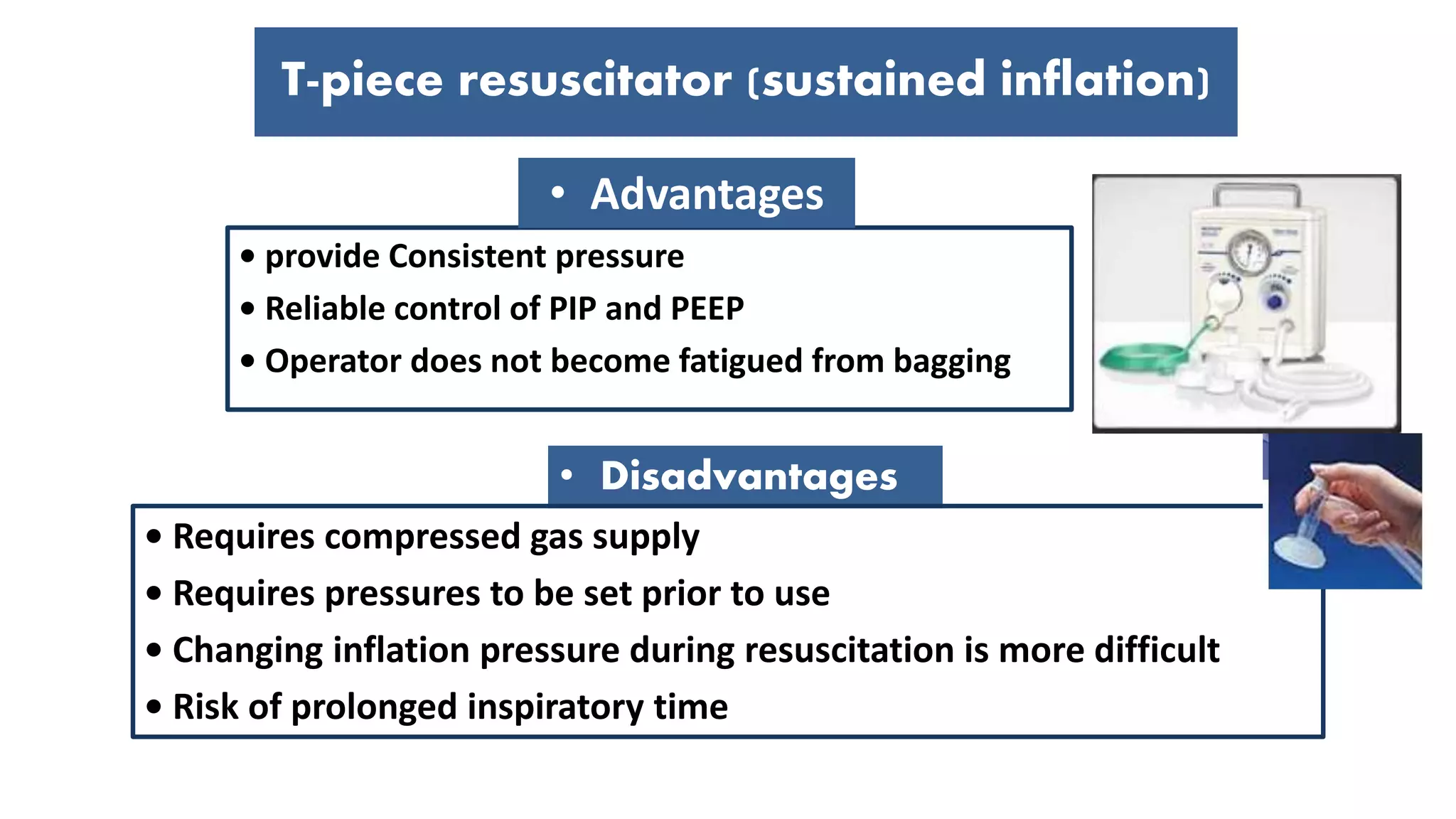




















This document provides guidance on positive pressure ventilation for newborn resuscitation. It discusses when PPV should be initiated, components of PPV including PIP, PEEP and flow rate. Three main types of resuscitation devices are described - self-inflating bag, flow-inflating bag and T-piece resuscitator. Key steps for preparing the resuscitation equipment and positioning the newborn are outlined. Intubation is discussed as an alternative to mask ventilation in certain situations. The document concludes with recommendations on oxygen use and monitoring during newborn resuscitation.


















































































