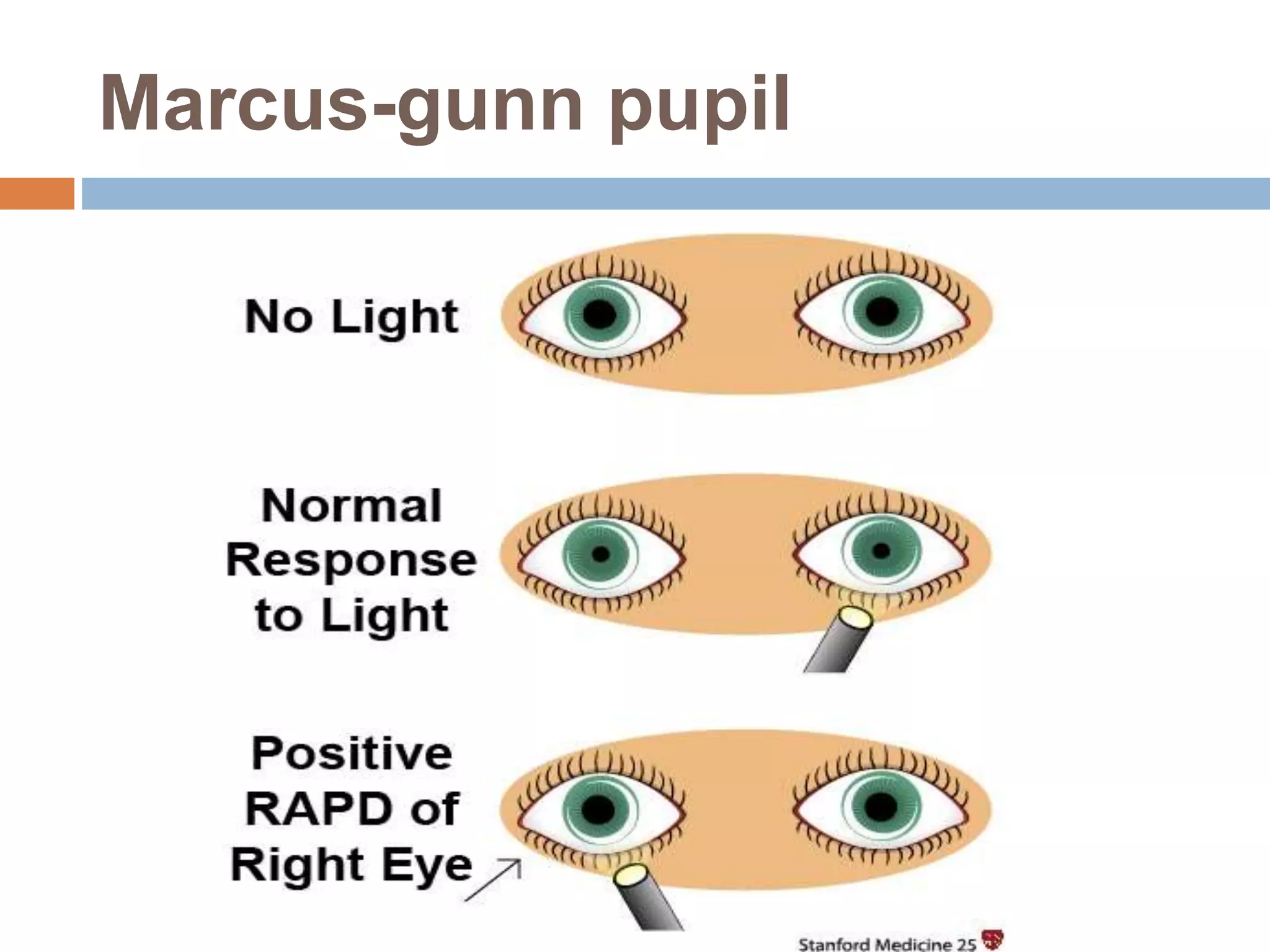
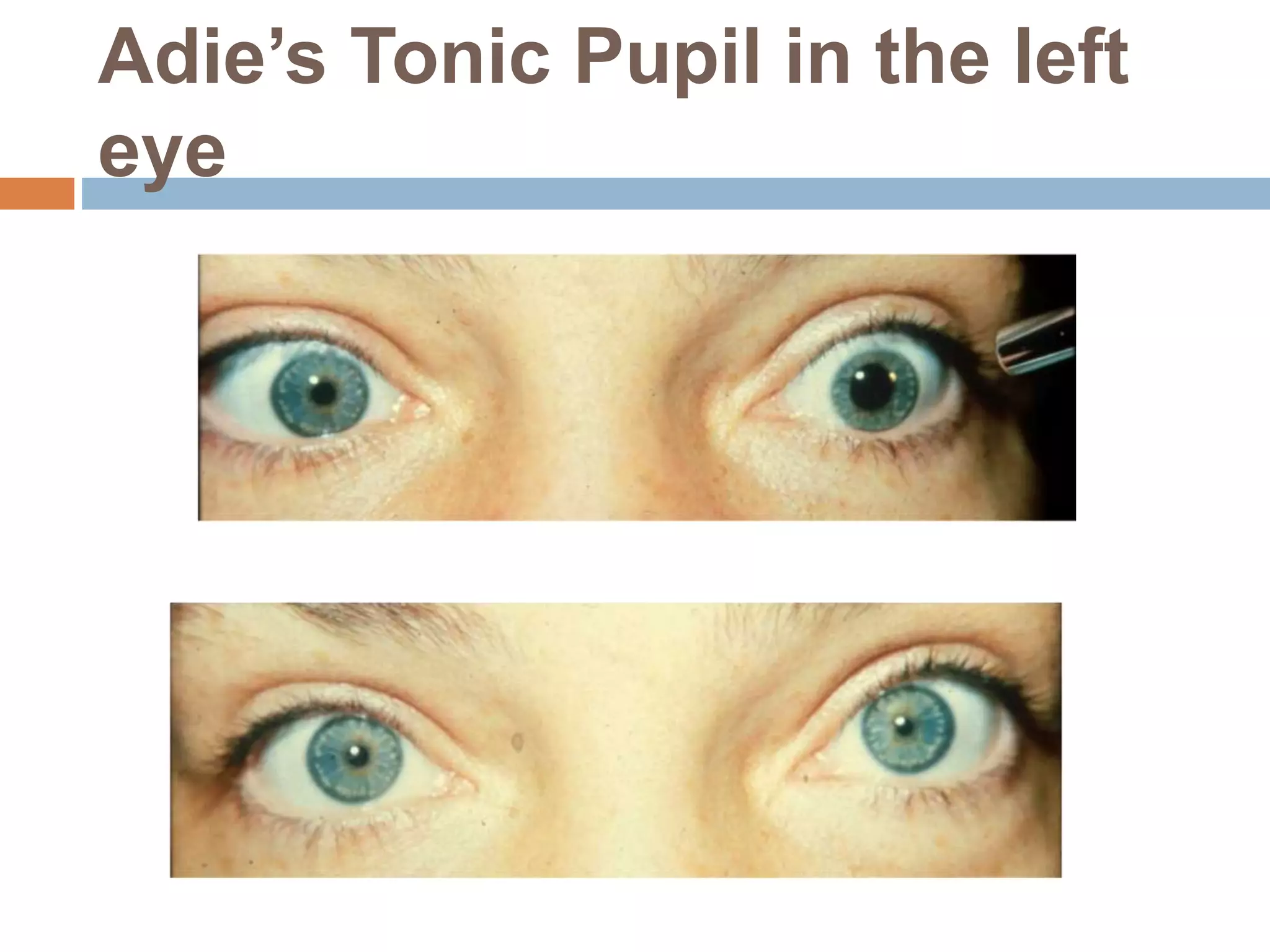
The document discusses various abnormalities of the pupil, including anisocoria, Marcus-Gunn pupil, and congenital conditions such as aniridia and iris coloboma. It outlines the features, differential diagnoses, and management strategies for several conditions affecting pupillary reflexes and structure. The document also highlights the impact of neurological disorders on pupil function, detailing conditions like Horner's syndrome and Adie's tonic pupil.