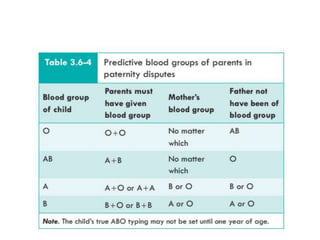
The document provides an overview of blood groups and blood typing systems. It discusses the history and discovery of blood groups, the ABO and Rh blood typing systems, inheritance of blood groups, clinical applications like blood transfusions and preventing hemolytic disease of the newborn. It describes the antigens and antibodies involved in blood typing, determining blood groups, population distributions of blood groups, and precautions for blood transfusions.