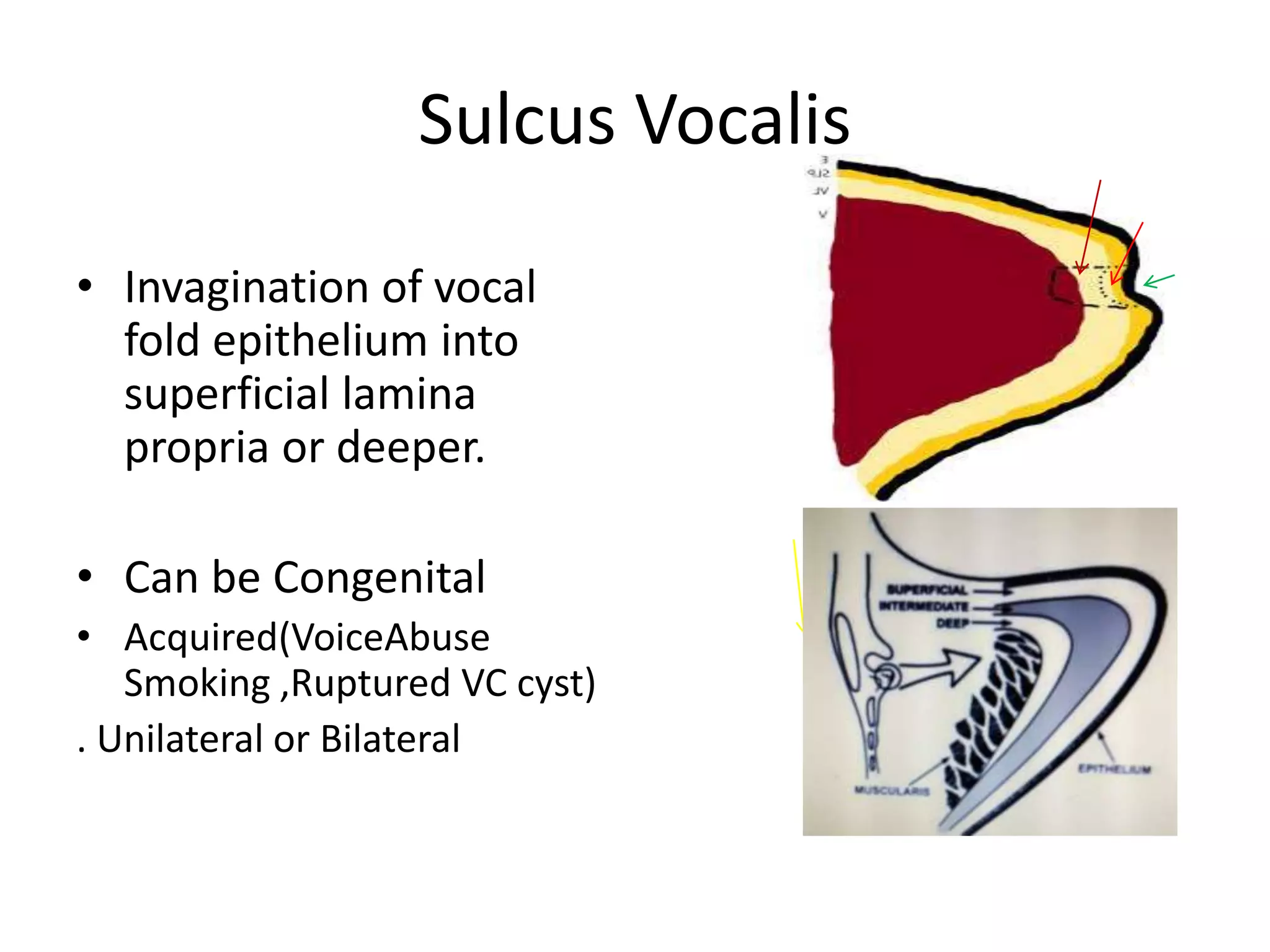
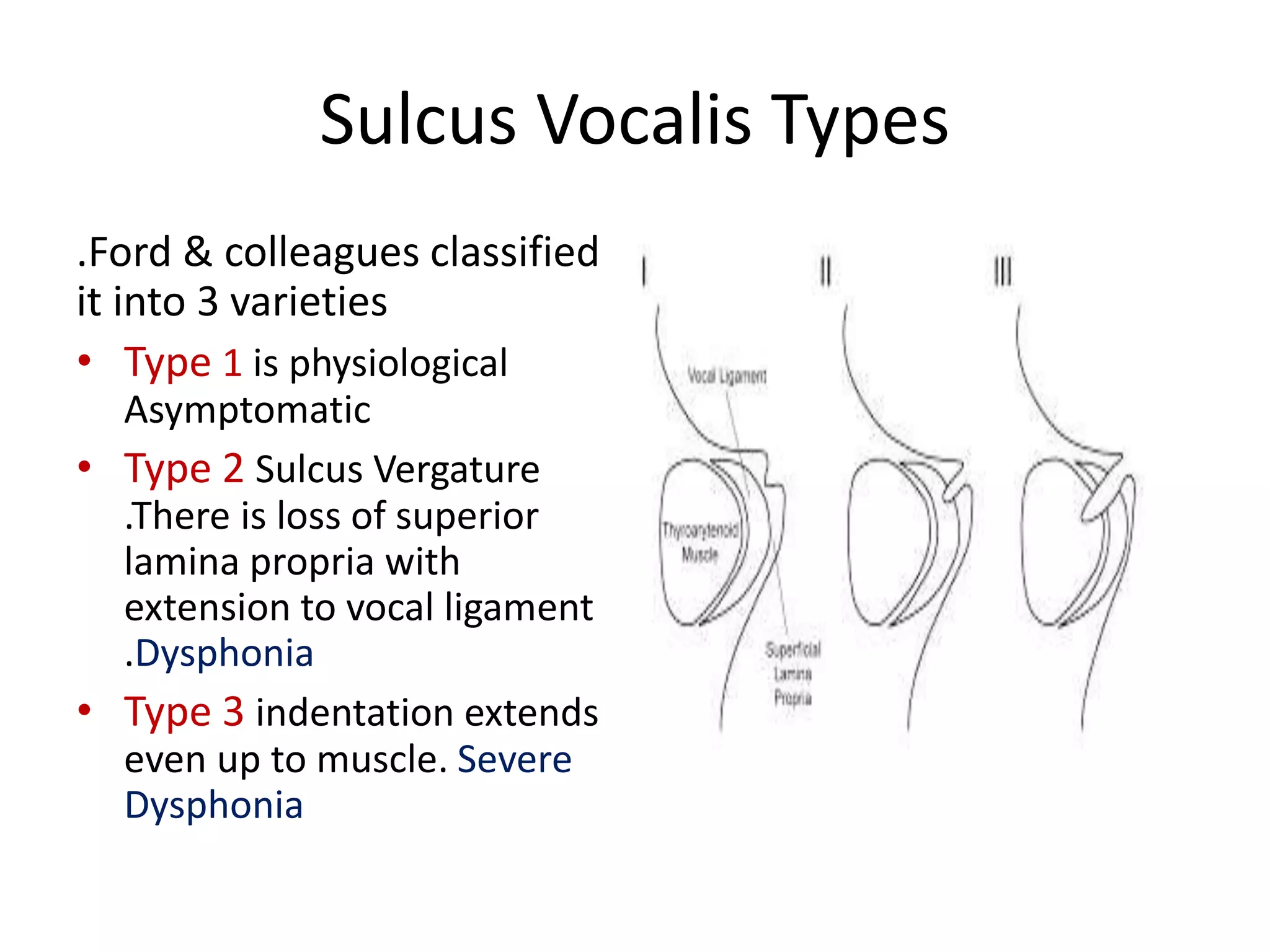
The document discusses sulcus vocalis, a condition involving the invagination of vocal fold epithelium, which can be congenital or acquired and leads to poor vocal fold function. It classifies the condition into three types based on severity and provides a stepwise treatment approach ranging from voice therapy to surgical interventions. The information is based on personal experience at Choithram Hospital and is intended for medical students and ENT postgraduates.