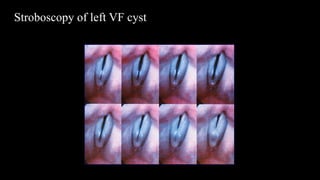
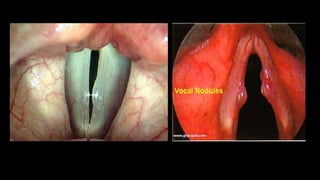
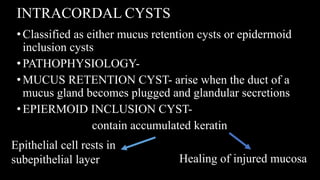
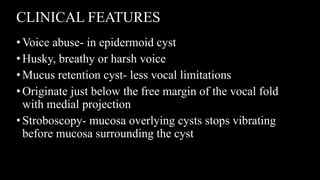
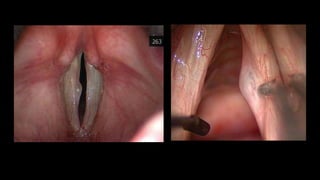
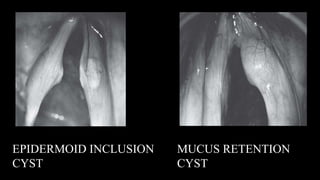
This document provides information on benign mucosal lesions of the larynx, including their etiology, clinical presentation, diagnosis, and management. The main lesions discussed are vocal fold nodules, polyps, cysts, fibrous masses, and scar tissue. Vocal fold nodules are typically caused by vocal hyperfunction and present with hoarseness and vocal fatigue. Polyps often arise from vocal hemorrhage during exertion. Intracordal cysts can be mucus retention or epidermoid in origin. These lesions are usually diagnosed via laryngoscopy and treated behaviorally or surgically via microlaryngeal techniques to remove the lesion while preserving healthy vocal fold tissue.