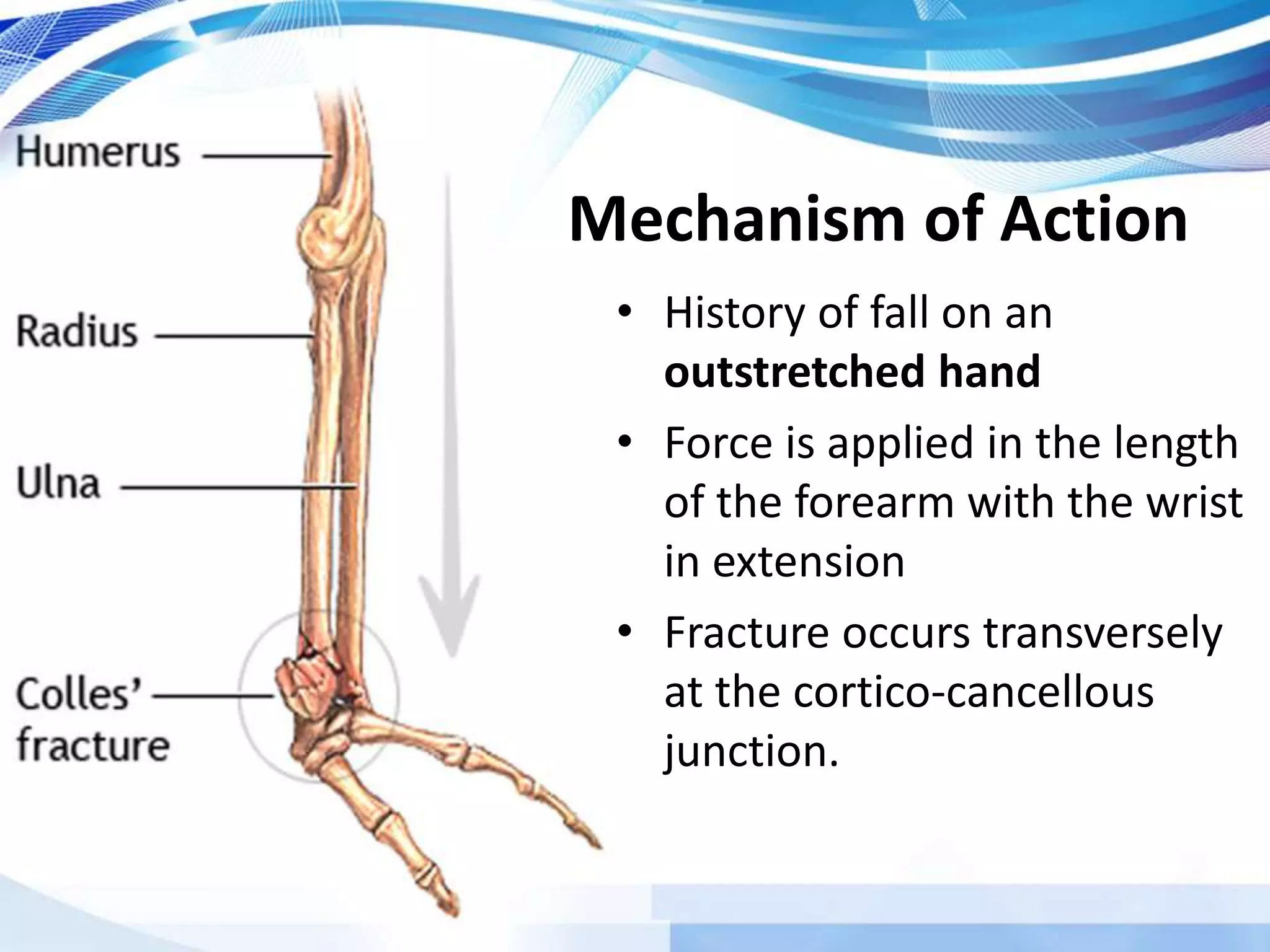
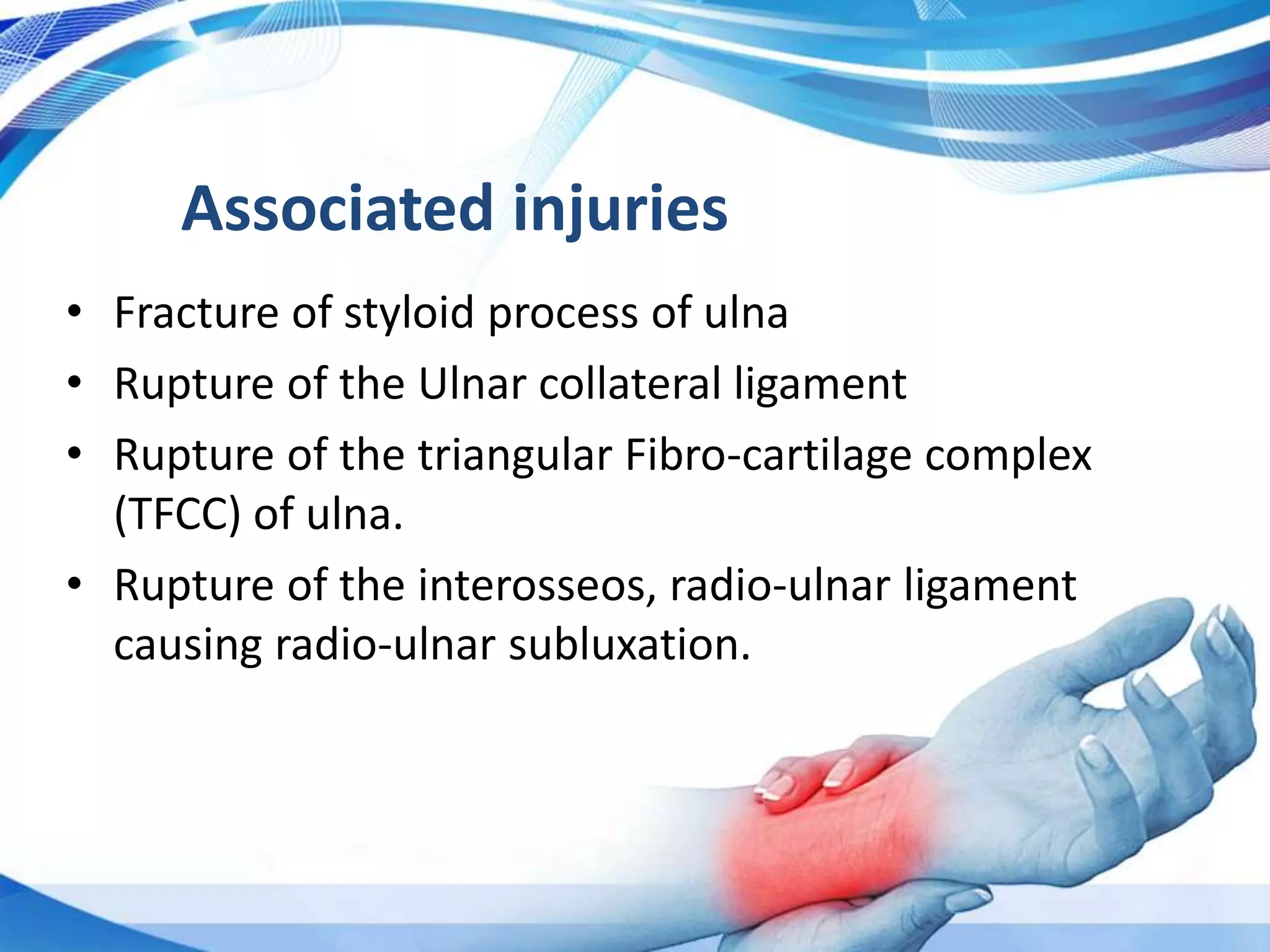
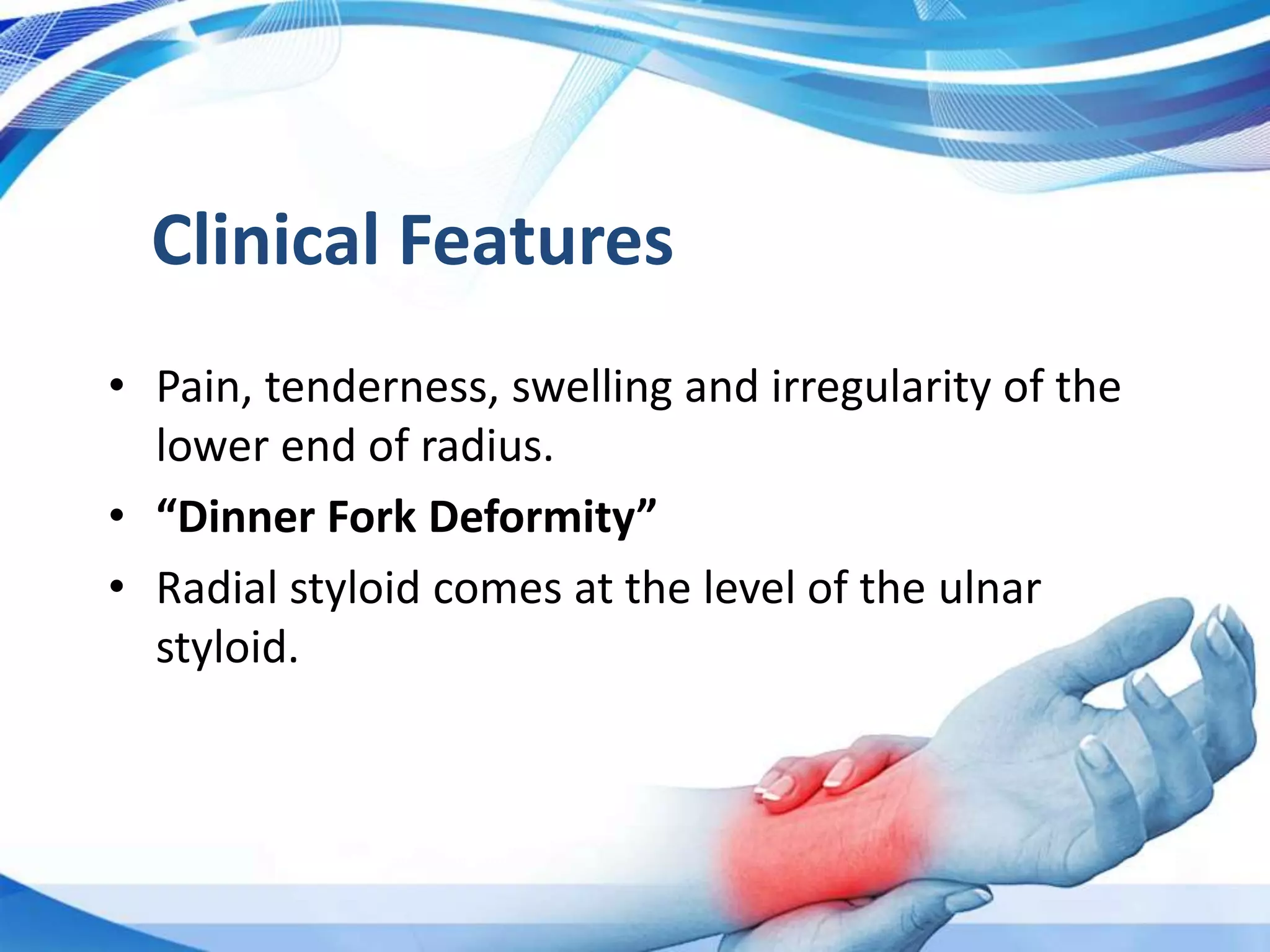
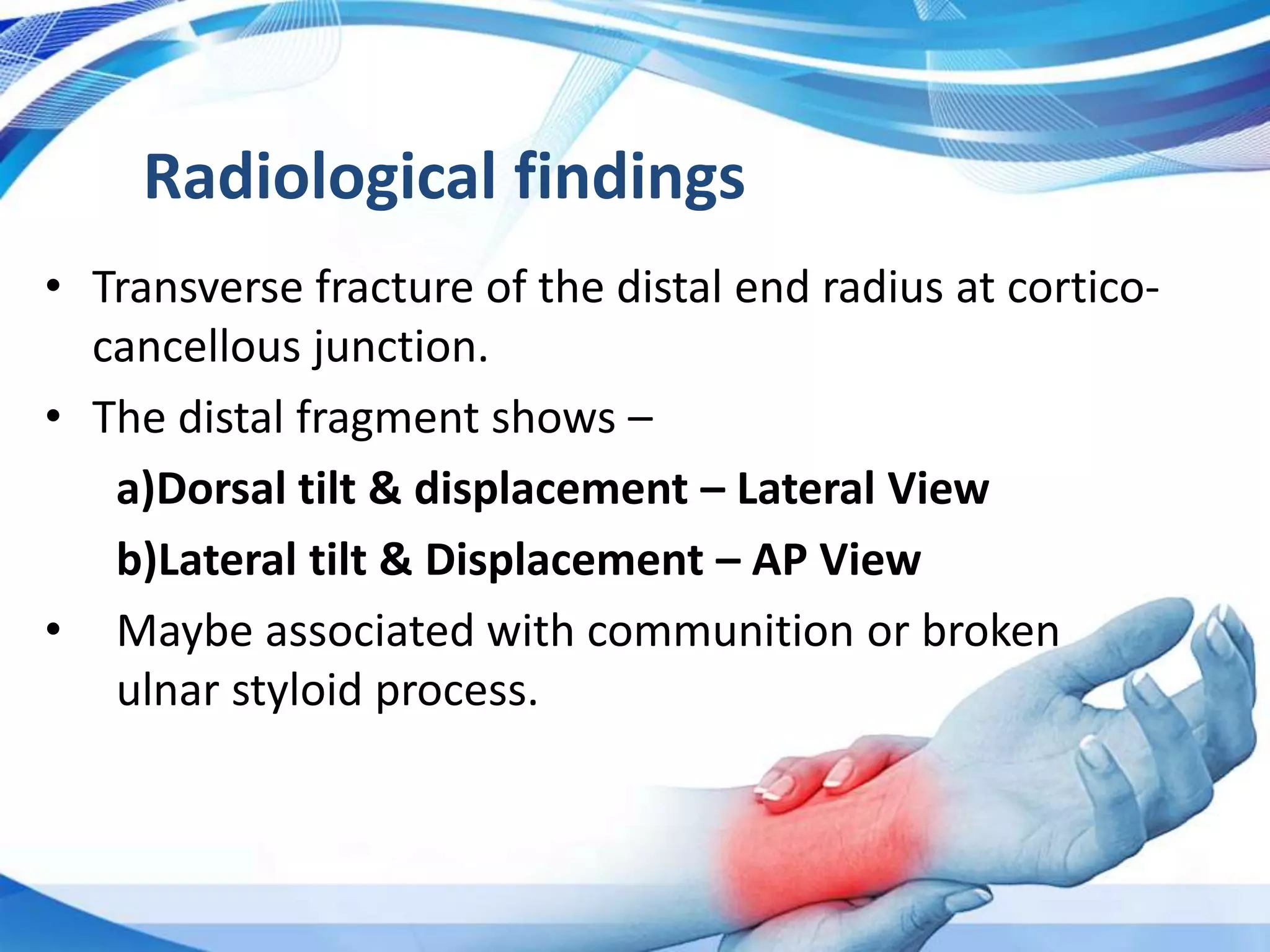
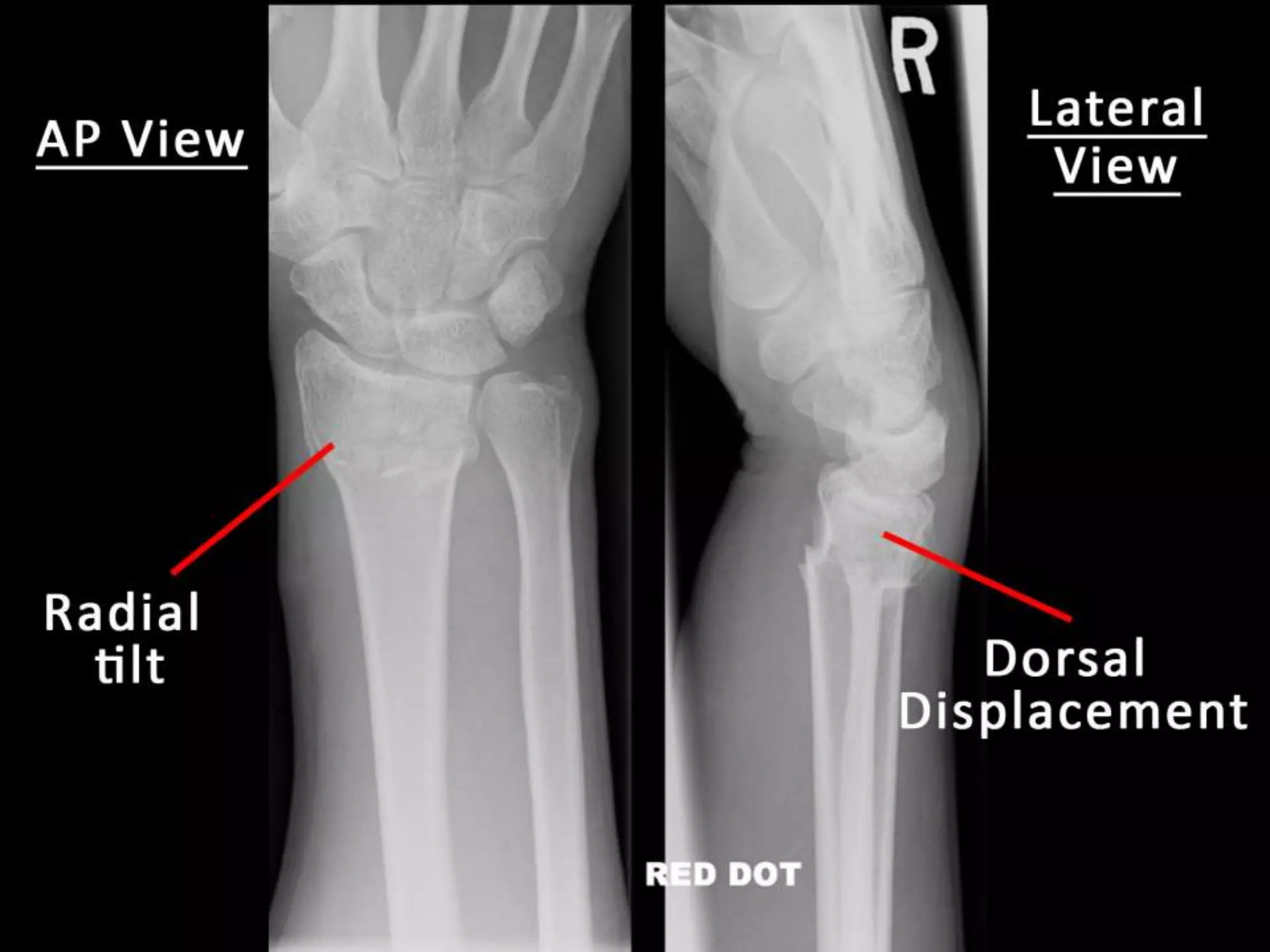
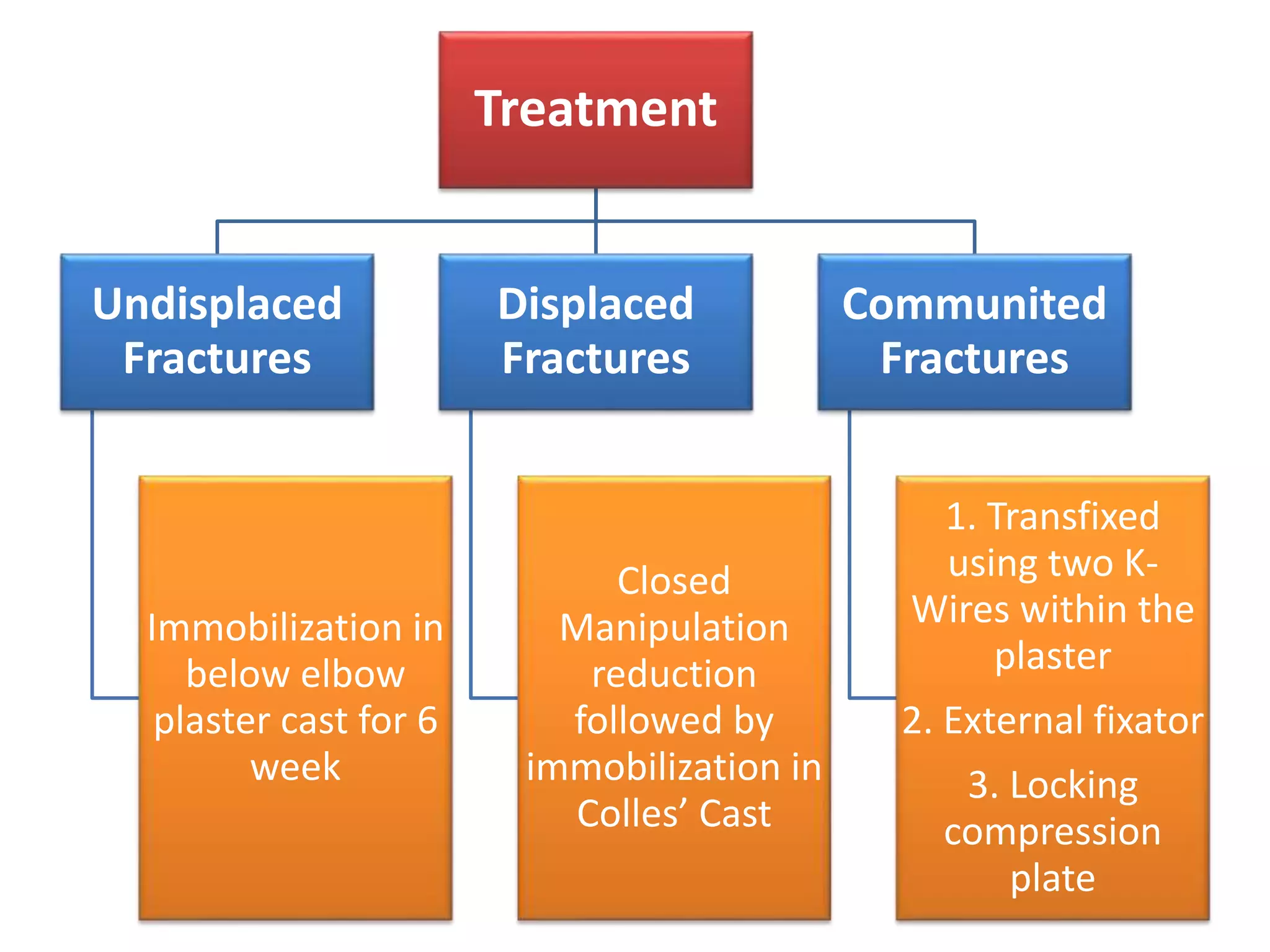
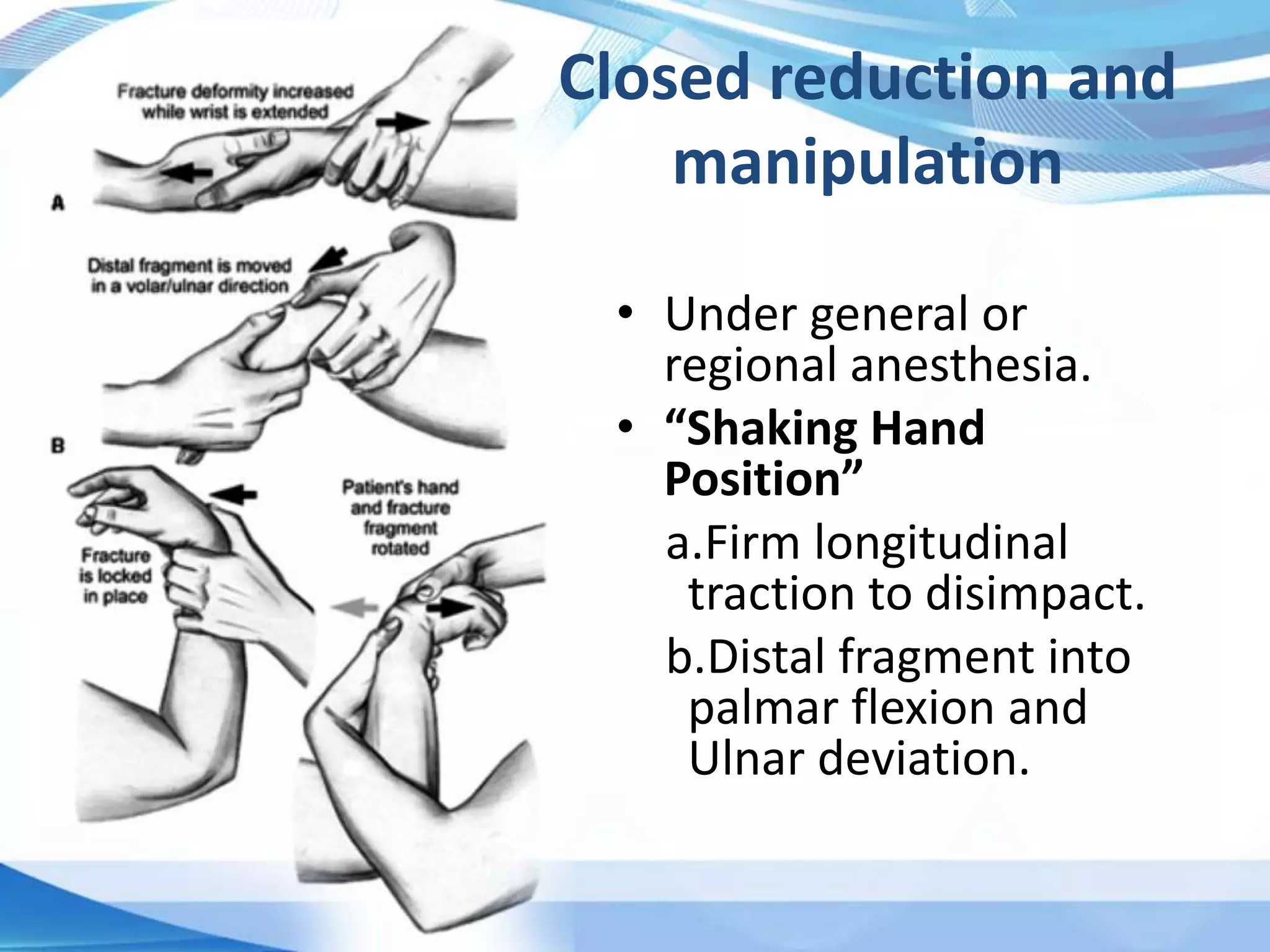
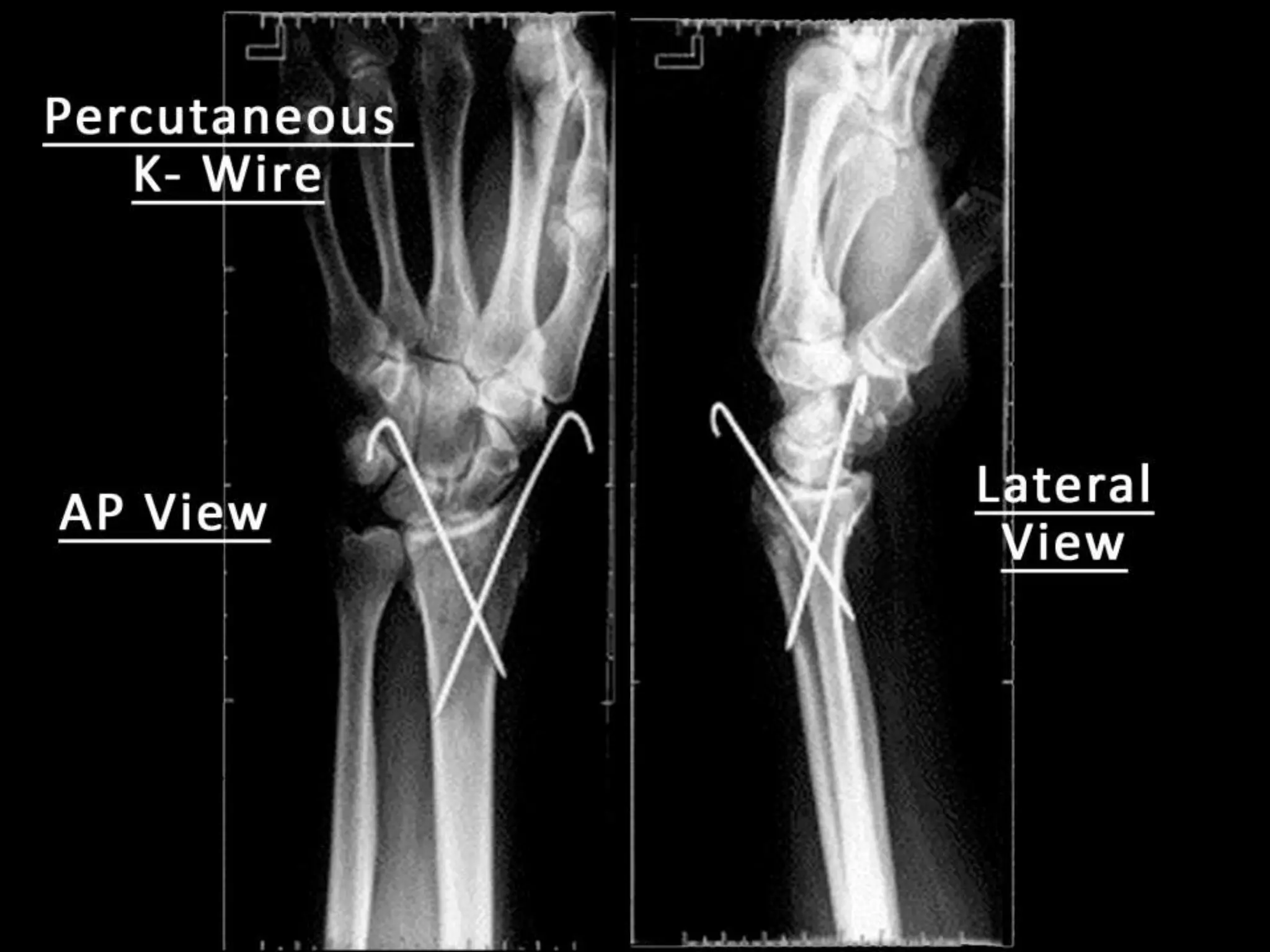
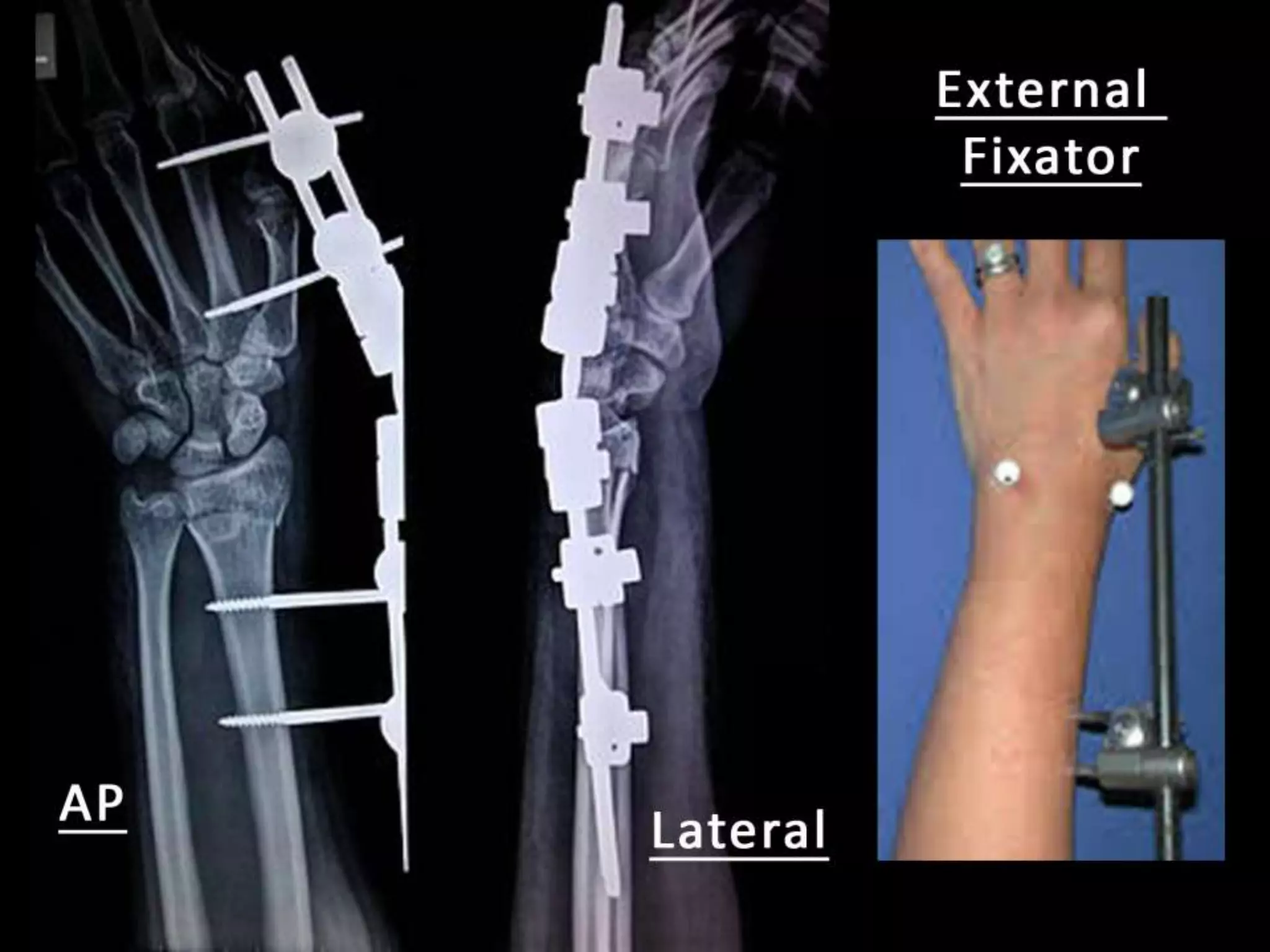
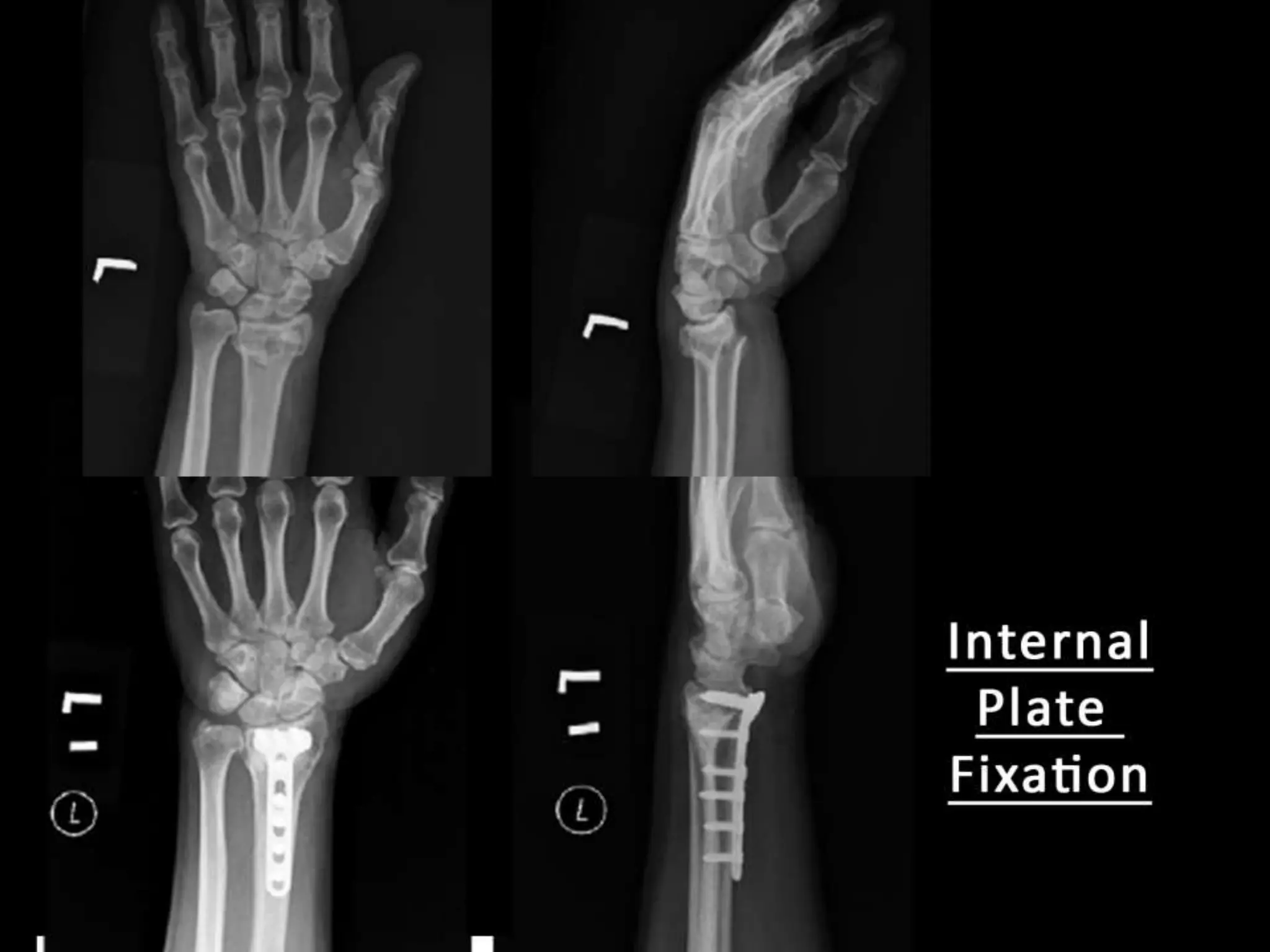
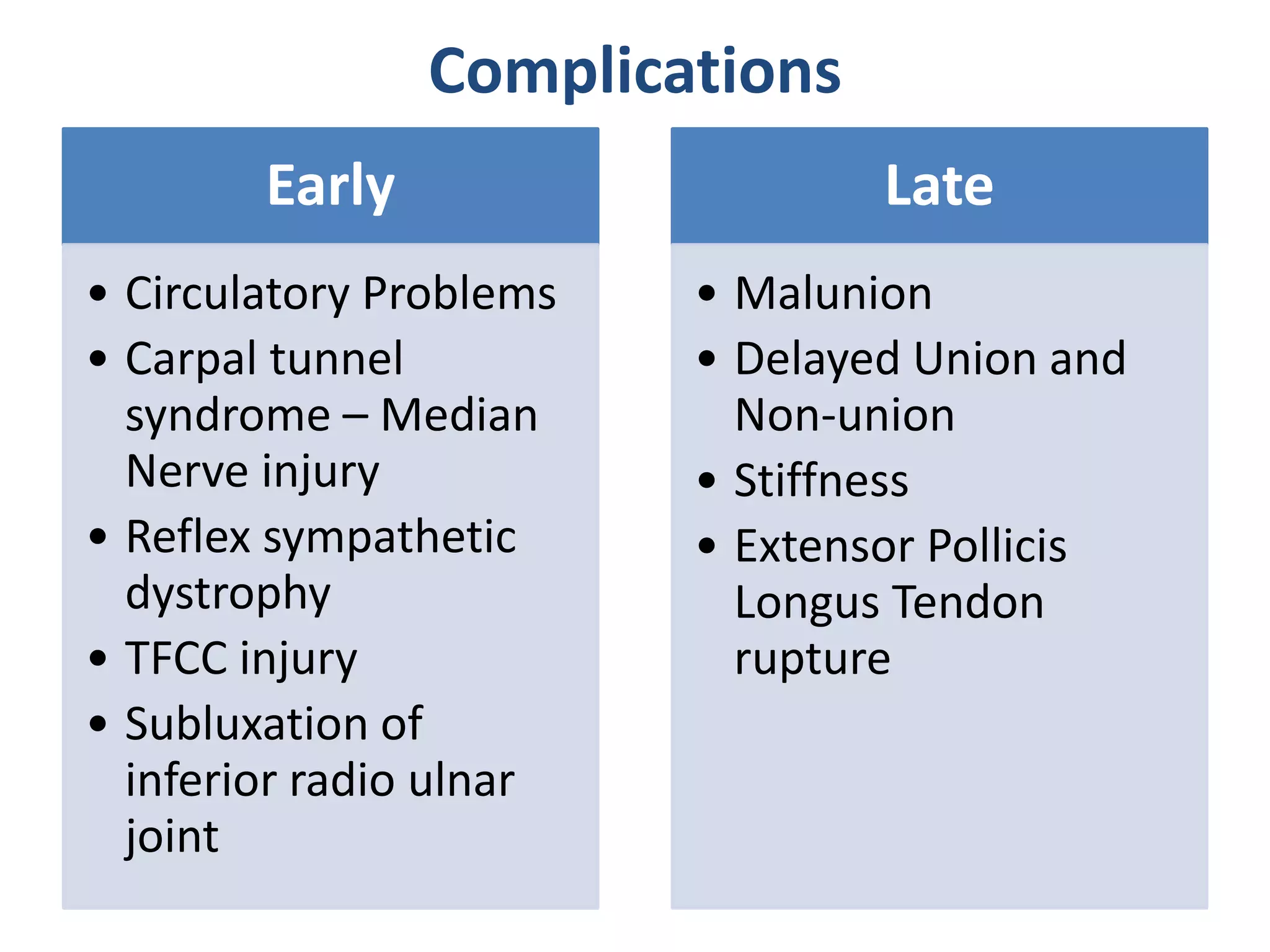
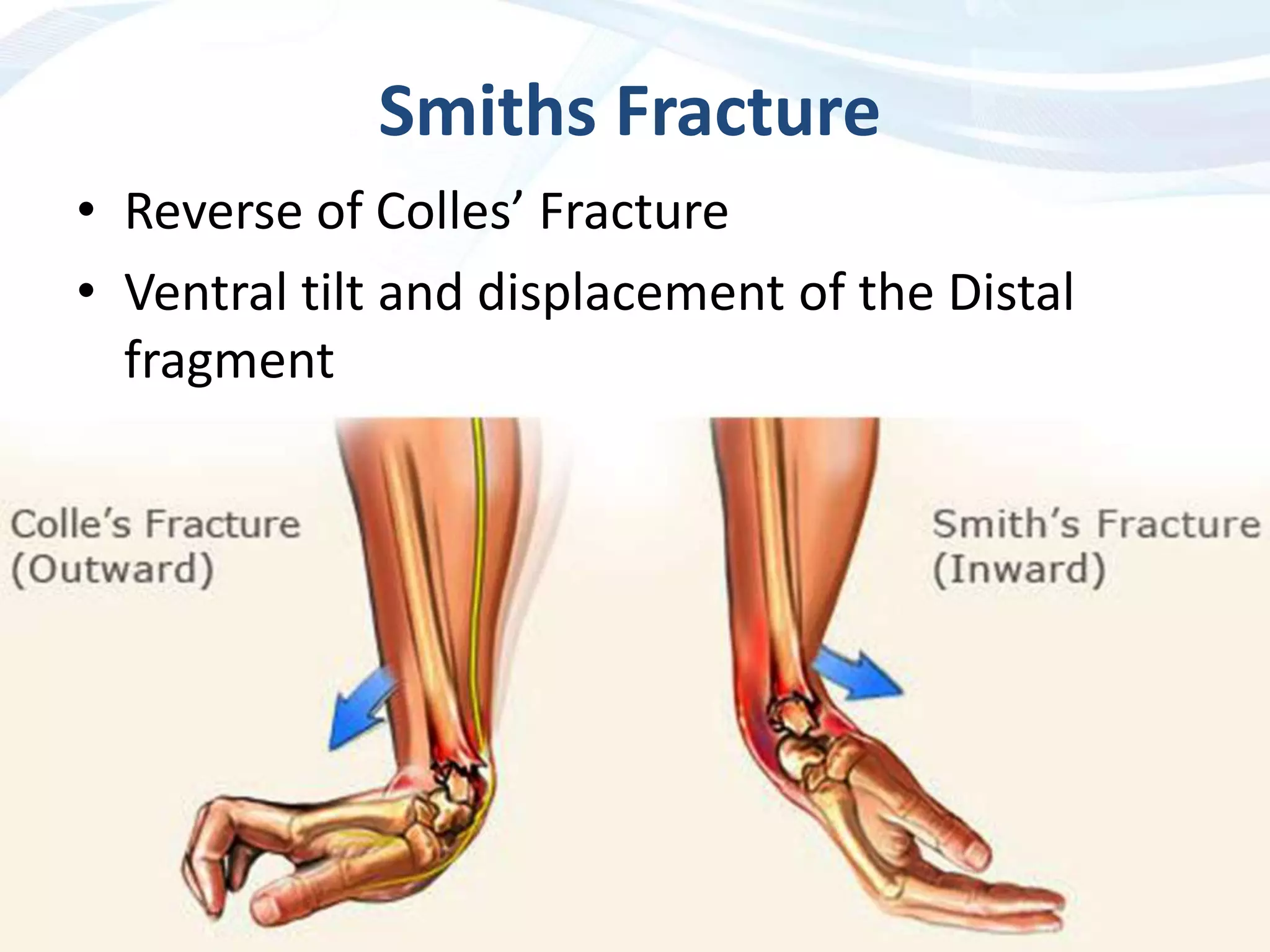
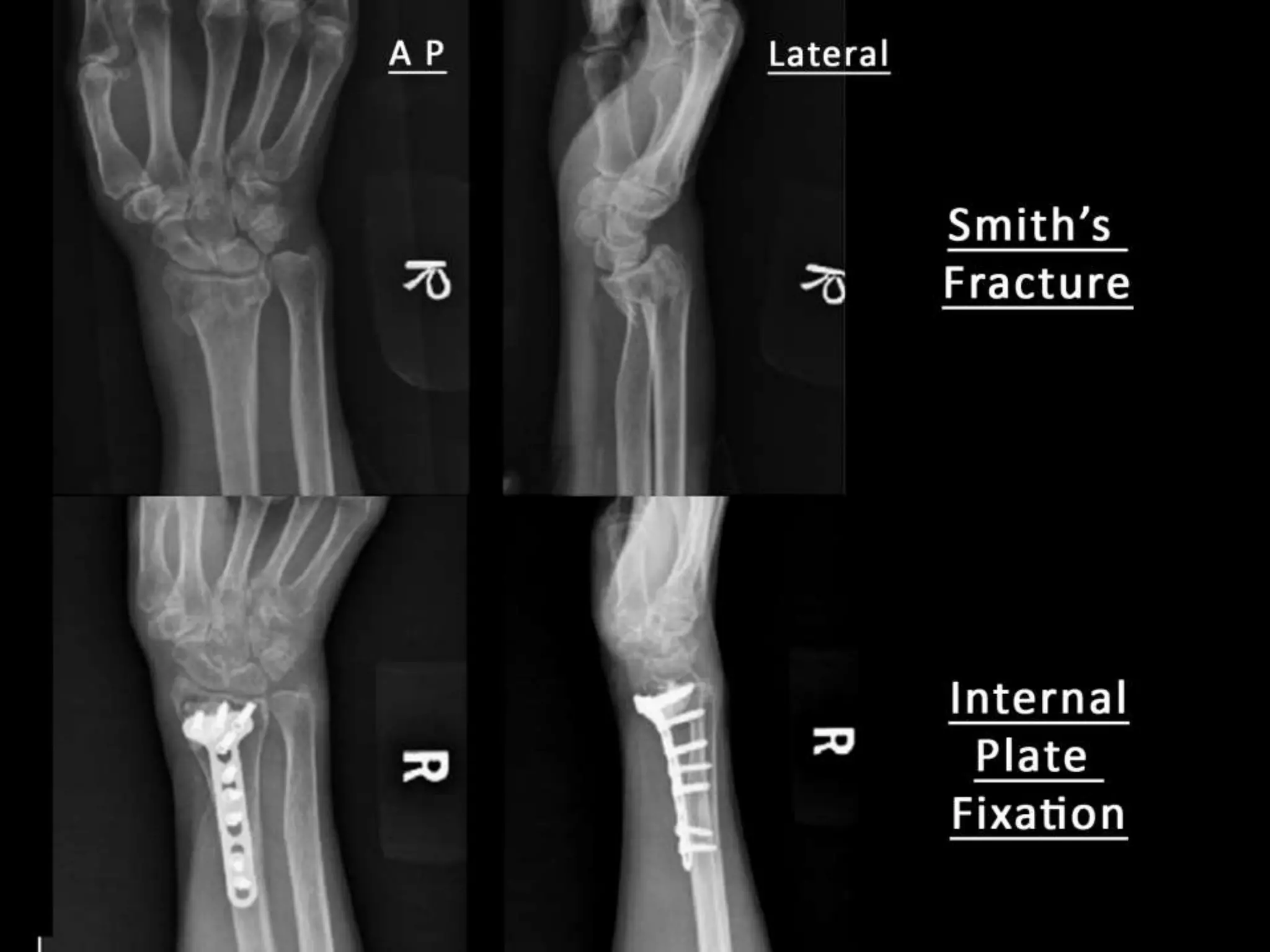
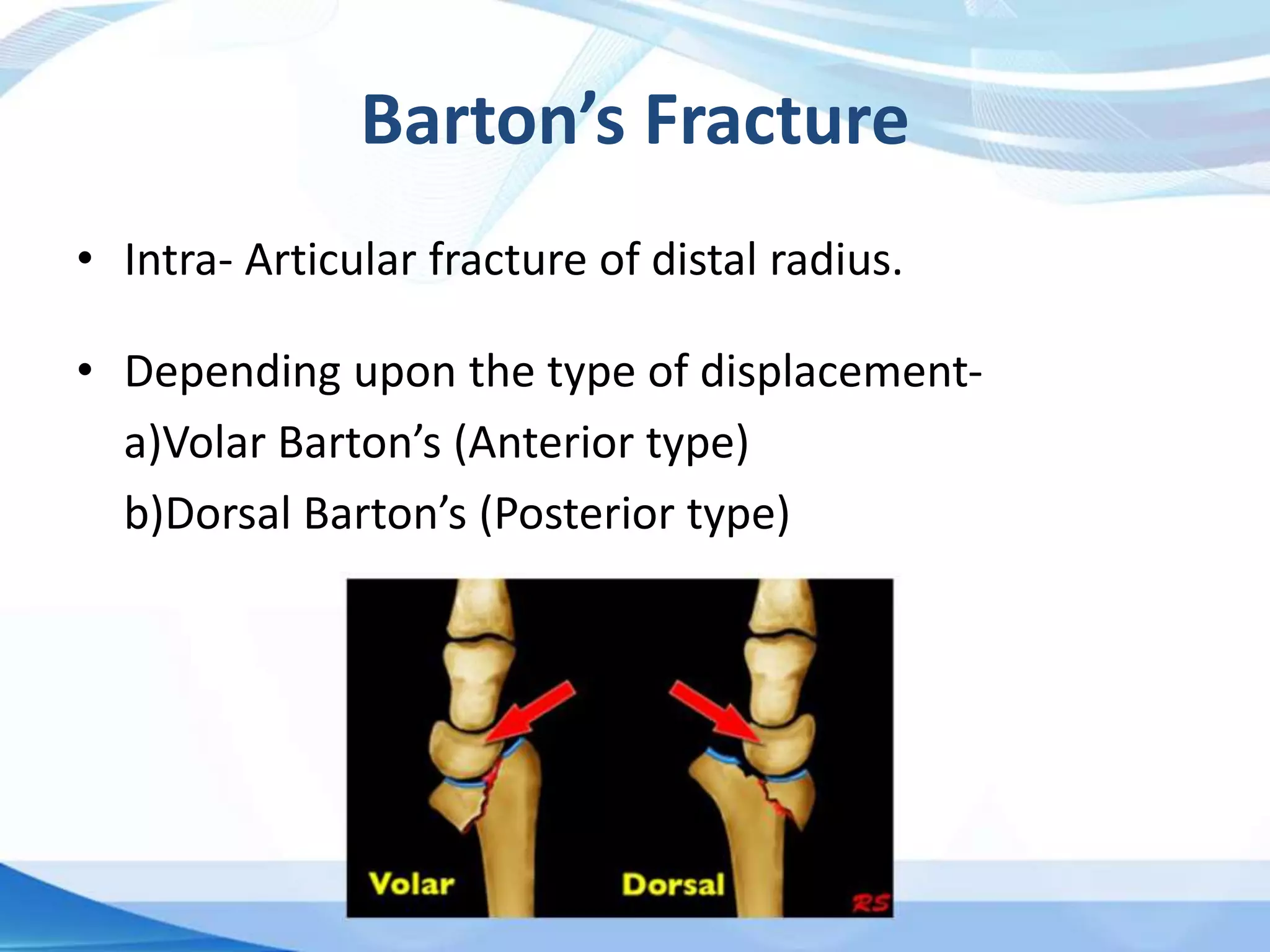
This document discusses various types of wrist fractures, including Colles', Smith's, and Barton's fractures, along with their mechanisms, clinical features, and treatments. Colles' fracture, the most common in the elderly, is characterized by dorsal displacement of the distal radius following a fall on an outstretched hand. Treatment varies based on fracture type, from immobilization to internal fixation, with potential complications outlined.