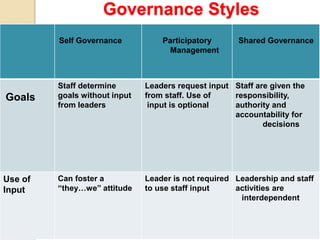
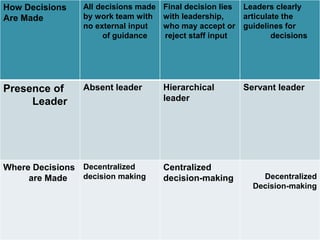
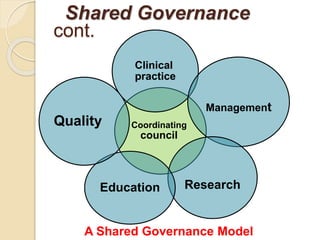
The document discusses shared governance in healthcare. It defines shared governance as a model where decision making power is shared between management, physicians, and nurses. This aims to empower nurses and improve the work environment. Under shared governance, councils are formed to make decisions related to areas like clinical practice, quality, education, research, and management. Barriers to implementing shared governance include resistance from managers accustomed to autocratic decision making and the significant long-term commitment required.