Shared Governance in Nursing: A dynamic facelift for empowered practice
The document discusses the concept of shared governance in nursing, emphasizing the need to transition from traditional hierarchical models to participative decision-making systems that empower nurses and promote collaboration. It outlines the key principles, benefits, and challenges associated with shared governance, as well as various models for its implementation. The piece highlights that successful integration requires ongoing education, support, and adaptation to specific organizational contexts.
Shared Governance in Nursing: A dynamic facelift for empowered practice
1.
SharedGovernance in
Nursing: Adynamicfaceliftfor
empoweredpractice
by: Nashrene Ahmed Raafat Elbar, RN, MAN
Submitted to:
Dr. David Hali de Jesus, RN, PgDip, FISQua
2.
DISCLOSURE
I do nothave any relevant financial
relationship with commercial interest to
disclose.
3.
OBJECTIVES:
Explore theconcept of Shared Governance
in Nursing
Discuss the principles and models underpinning
practice
Identify challenges and recommendations for
effective implementation
4.
2nd HGH -Pediatric Emergency Centers Nursing Symposium
School
Absente
eism
So why are we much interested?
Switching gears
towards a shared
governance
approach is driven
by certain
‘Push Factors’
(Green and Jordan, 2002)
5.
‘From Hierarchy toRelational Partnership’
There is a need to break from the
traditional hospital governance where
nurses have little power in a rigid formal
hierarchical bureaucracy. `
6.
Traditional hierarchical
governance model
Governance’smost needed upgrade
FROM THIS TO THIS
Participative decision-making
Position-based
Limited staff
input
Hierarchical
communication
WE-THEY work
environment
Divided goals
and purpose
(Guanci, 2018)
7.
2nd HGH -Pediatric Emergency Centers Nursing Symposium
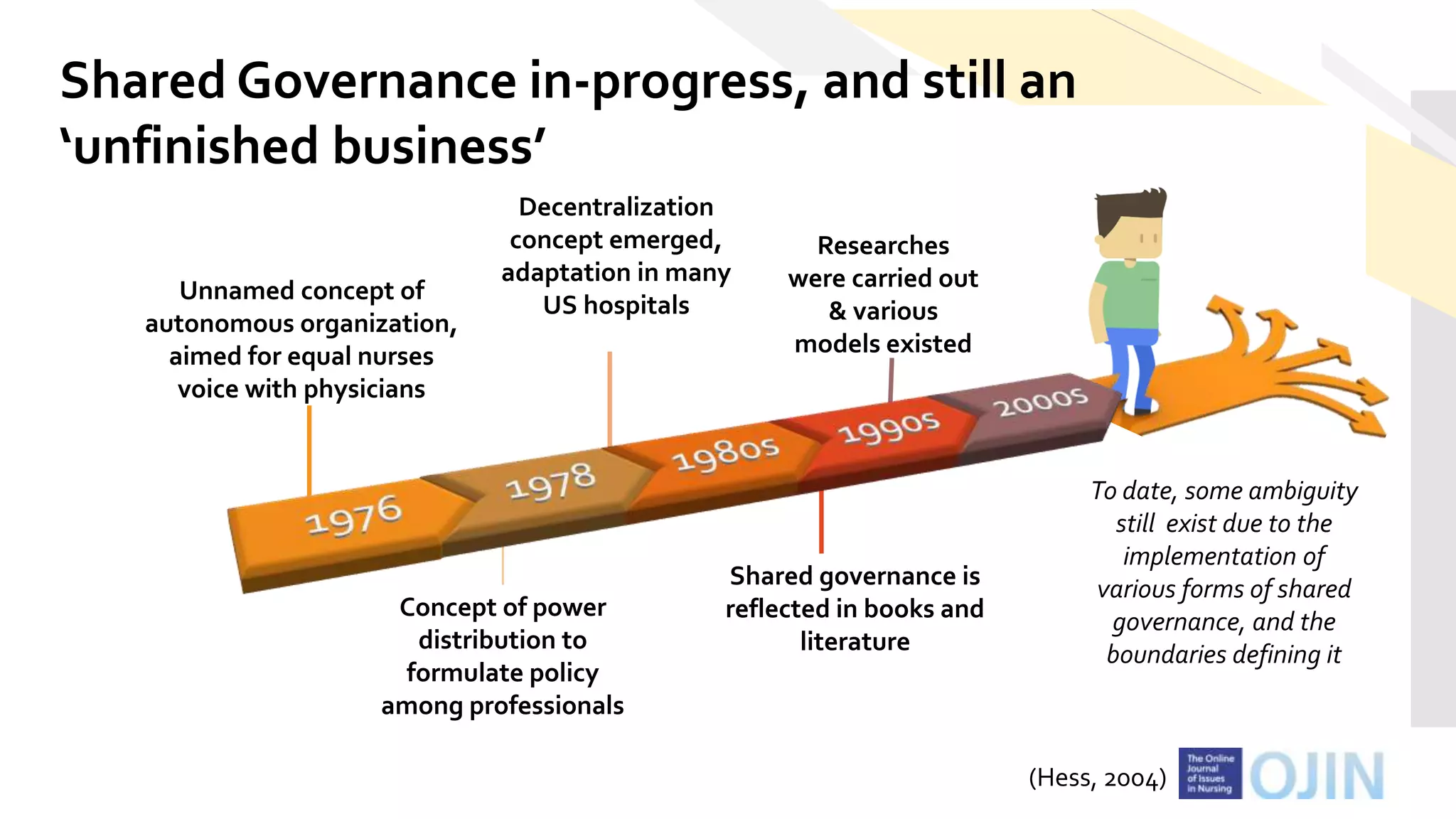
Unnamed concept of
autonomous organization,
aimed for equal nurses
voice with physicians
Decentralization
concept emerged,
adaptation in many
US hospitals
Concept of power
distribution to
formulate policy
among professionals
Researches
were carried out
& various
models existed
Shared governance is
reflected in books and
literature
Shared Governance in-progress, and still an
‘unfinished business’
To date, some ambiguity
still exist due to the
implementation of
various forms of shared
governance, and the
boundaries defining it
(Hess, 2004)
8.
Key features ofShared Governance:
autonomy
independence in practice
accountability
empowerment
participation
collaboration
9.
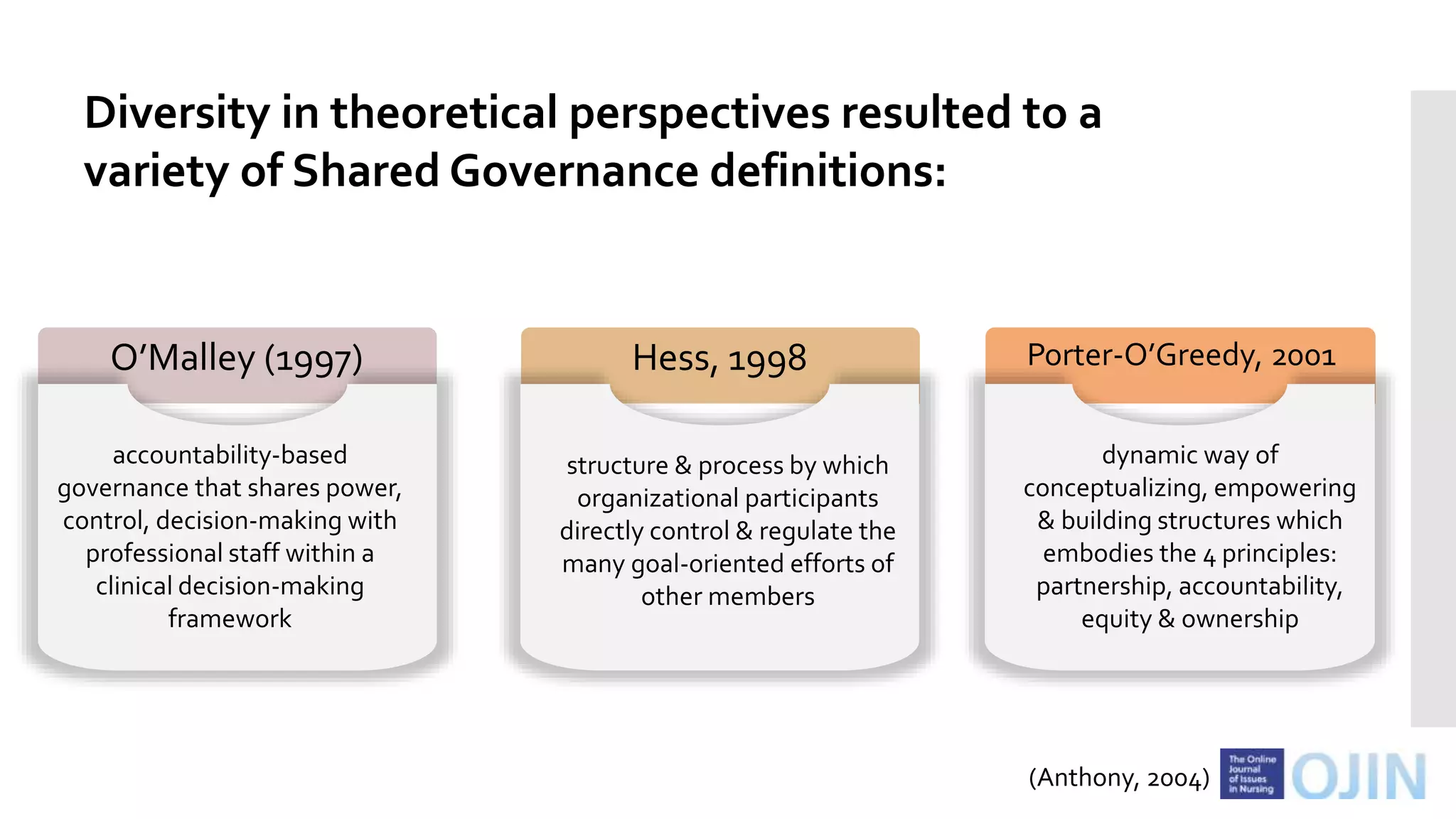
Diversity in theoreticalperspectives resulted to a
variety of Shared Governance definitions:
O’Malley (1997) Hess, 1998 Porter-O’Greedy, 2001
accountability-based
governance that shares power,
control, decision-making with
professional staff within a
clinical decision-making
framework
structure & process by which
organizational participants
directly control & regulate the
many goal-oriented efforts of
other members
dynamic way of
conceptualizing, empowering
& building structures which
embodies the 4 principles:
partnership, accountability,
equity & ownership
(Anthony, 2004)
10.
In simpler terms,Shared Governance:
is an organizational strategy by which
nurses can advocate for, and manage
their professional role with greater
degree of autonomy
its strategy is focused on partnership
between the organization and the
individual nurse
creates an environment where
professional accountability is respected
and encouraged
“where staff nurses move from the bottom to the center of the organization”
(Church et al, 2008)
11.
2nd HGH -Pediatric Emergency Centers Nursing Symposium
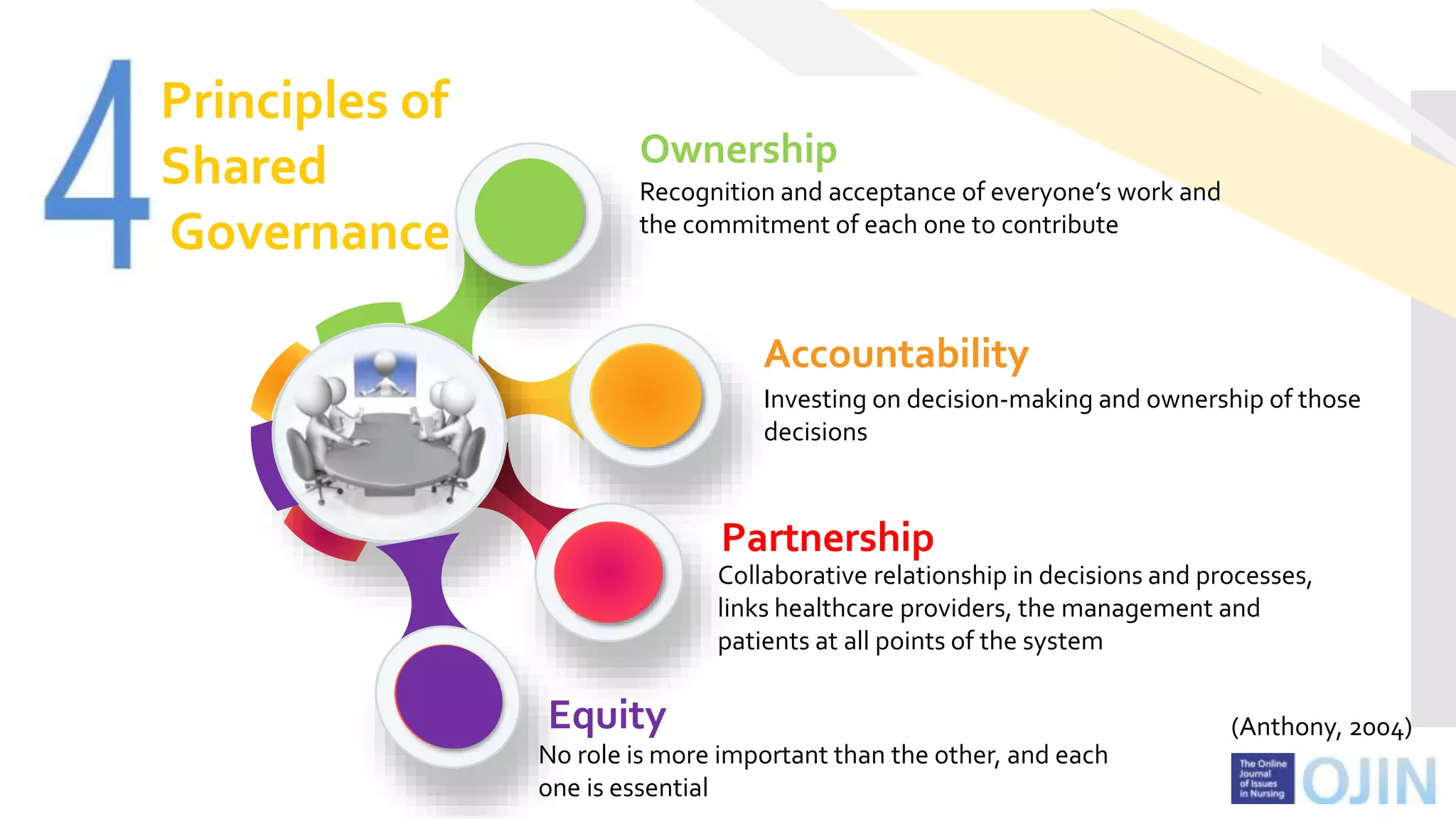
Principles of
Shared
Governance
Partnership
Collaborative relationship in decisions and processes,
links healthcare providers, the management and
patients at all points of the system
Equity
No role is more important than the other, and each
one is essential
Accountability
Investing on decision-making and ownership of those
decisions
Ownership
Recognition and acceptance of everyone’s work and
the commitment of each one to contribute
(Anthony, 2004)
12.
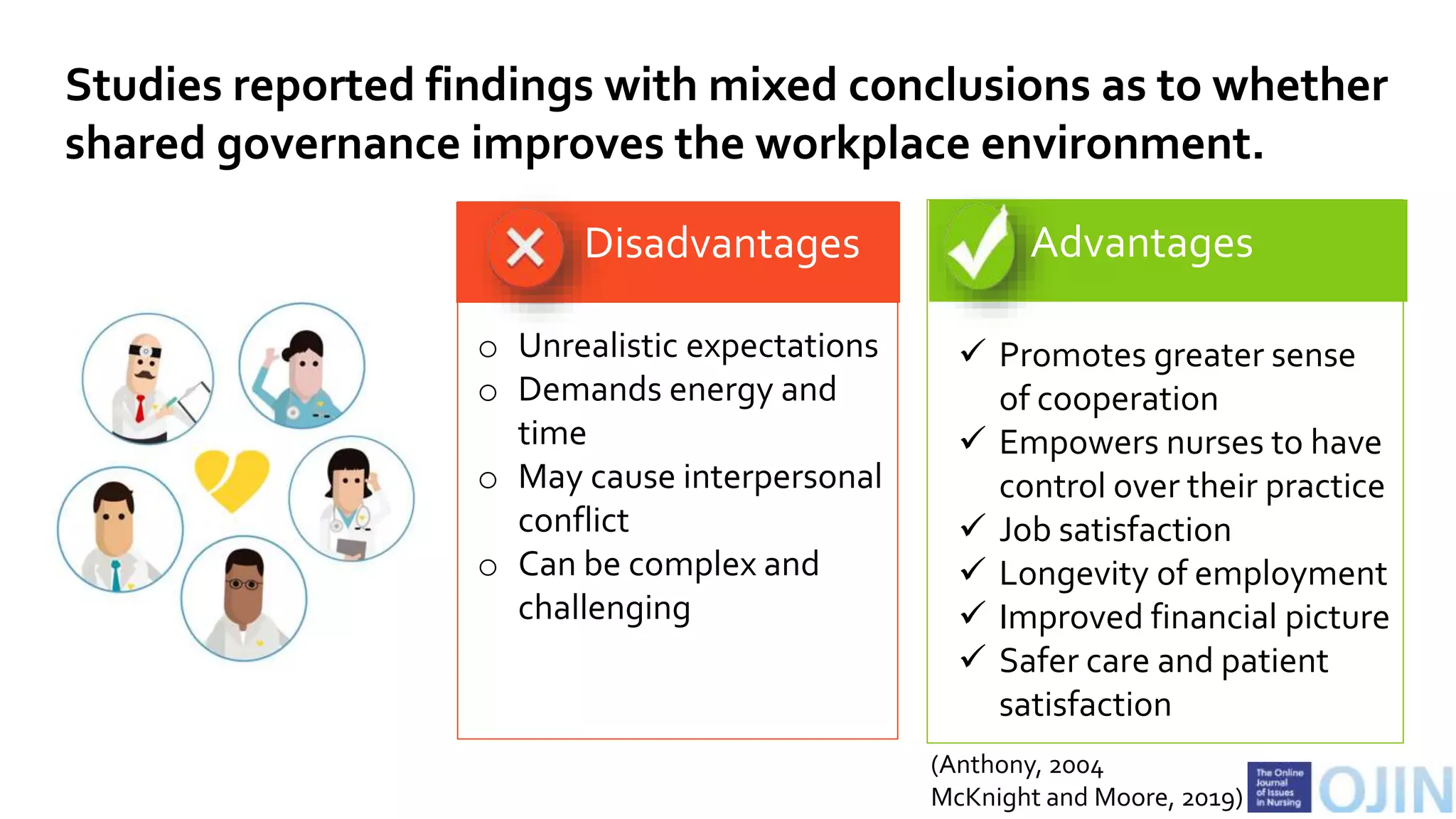
Advantages
Promotes greatersense
of cooperation
Empowers nurses to have
control over their practice
Job satisfaction
Longevity of employment
Improved financial picture
Safer care and patient
satisfaction
Disadvantages
o Unrealistic expectations
o Demands energy and
time
o May cause interpersonal
conflict
o Can be complex and
challenging
Studies reported findings with mixed conclusions as to whether
shared governance improves the workplace environment.
(Anthony, 2004
McKnight and Moore, 2019)
13.
2nd HGH -Pediatric Emergency Centers Nursing Symposium
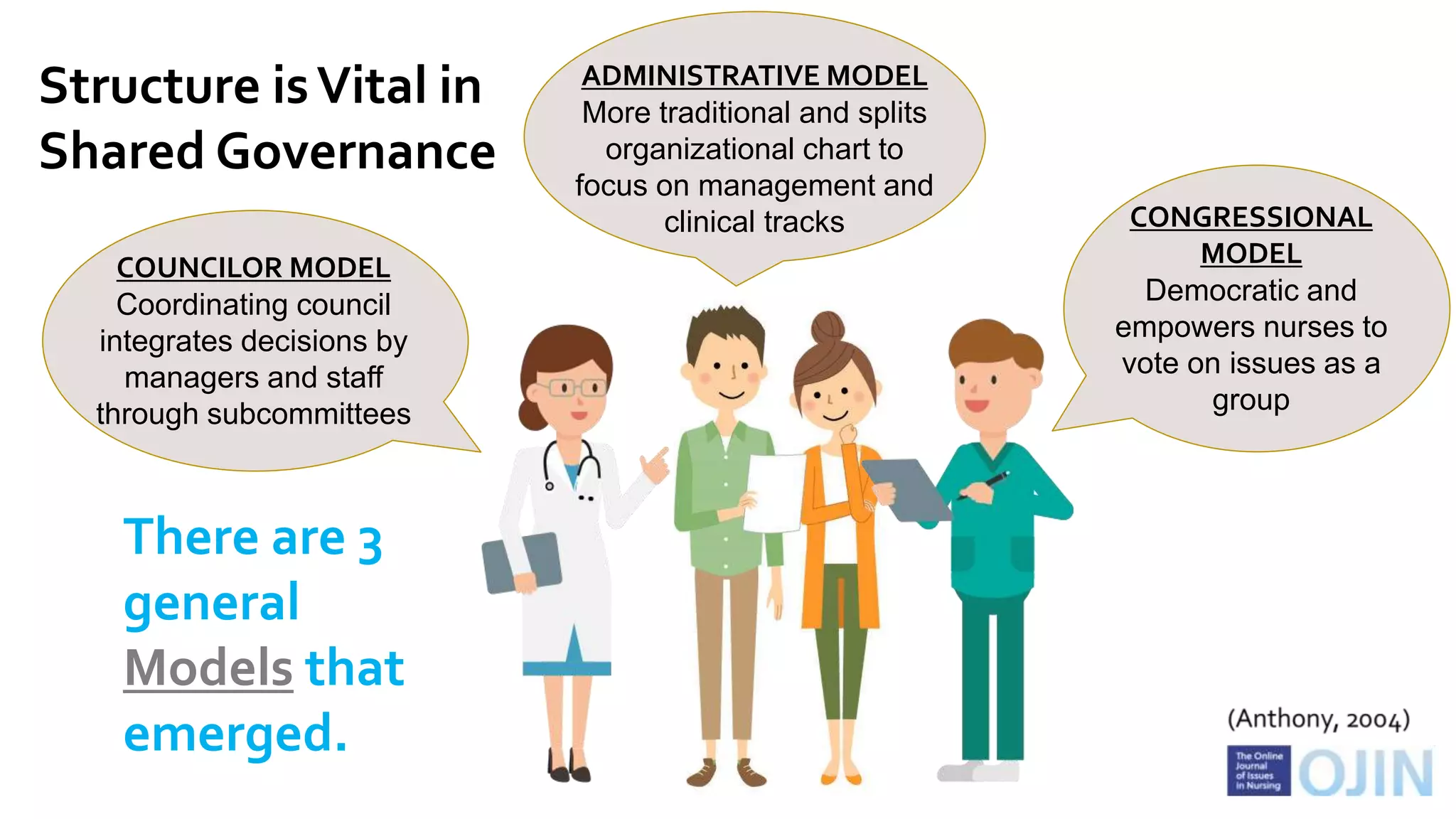
COUNCILOR MODEL
Coordinating council
integrates decisions by
managers and staff
through subcommittees
ADMINISTRATIVE MODEL
More traditional and splits
organizational chart to
focus on management and
clinical tracks CONGRESSIONAL
MODEL
Democratic and
empowers nurses to
vote on issues as a
group
Structure isVital in
Shared Governance
There are 3
general
Models that
emerged.
14.
Shared Governance modelscan also be
categorized as:
WHOLE SYSTEMS SHARED COVERNANCE
which involves all levels of the organization, including all
disciplines, departments and employees
NURSE SHARED GOVERNANCE
strategies are focused on partnership between the organization
and the nurse
PROFESSIONAL SHARED GOVERNANCE
Creation of teams of stakeholders that are focused on
realizing goals (*new concept)
(O’May and Buchan, 1999)
15.
How can nursesstep-up and engage in Shared Governance?
?
?? ?
16.
Shared Governance actions:
Accountability
-Nurses recognize current workplace issues and
seeks support needed to address these concerns.
- Nurses participate in development of practice
standards and quality assurance monitoring.
Empowerment
- Nurses voice is strengthened by involving them in
workplace decisions that affect patient care, such
as participation in unit-based councils.
17.
Shared Governance actions:
Conflictresolution and patient
advocacy
- Nurses participate in a non-hierararchial power,
interaction in work design.
- Decision support and conflict resolution is
available at the point of care delivery, and
conflict is resolved at the level where it occurs.
- Nurses speak up to improve practices that
ensures delivery of safe care.
18.
The implementation ofShared Governance is
not easy. It can be riddled with conceptual
ambiguity and resistance. Not all will share
the enthusiasm to this wonderful innovation.
19.
2nd HGH -Pediatric Emergency Centers Nursing Symposium
The journey is long and
steep. Lack of opportunities
for staff to acquire skills
leads to disengagement and
frustration.
Shared Governance requires
constant revitalization and
renewal.
Lack of researches with
rigorous designs.
Evaluation of the
process and its effects
may be difficult.
Not every environment is
conducive to shared
governance.
Shared governance
may be exclusionary
and focus on goals of
a single profession.
Roadblocks to successful implementation
(Porter-O’Grady, 2019)
20.
How can wemake it better?
Establish consensus and clear
extent where governance exists
Conduct more researches
focused on outcomes (benefits
to nurses, patients and
organizations)
Reconcile gaps in theoretical
perspectives and variations in
implementation
Educate, educate, educate
21.
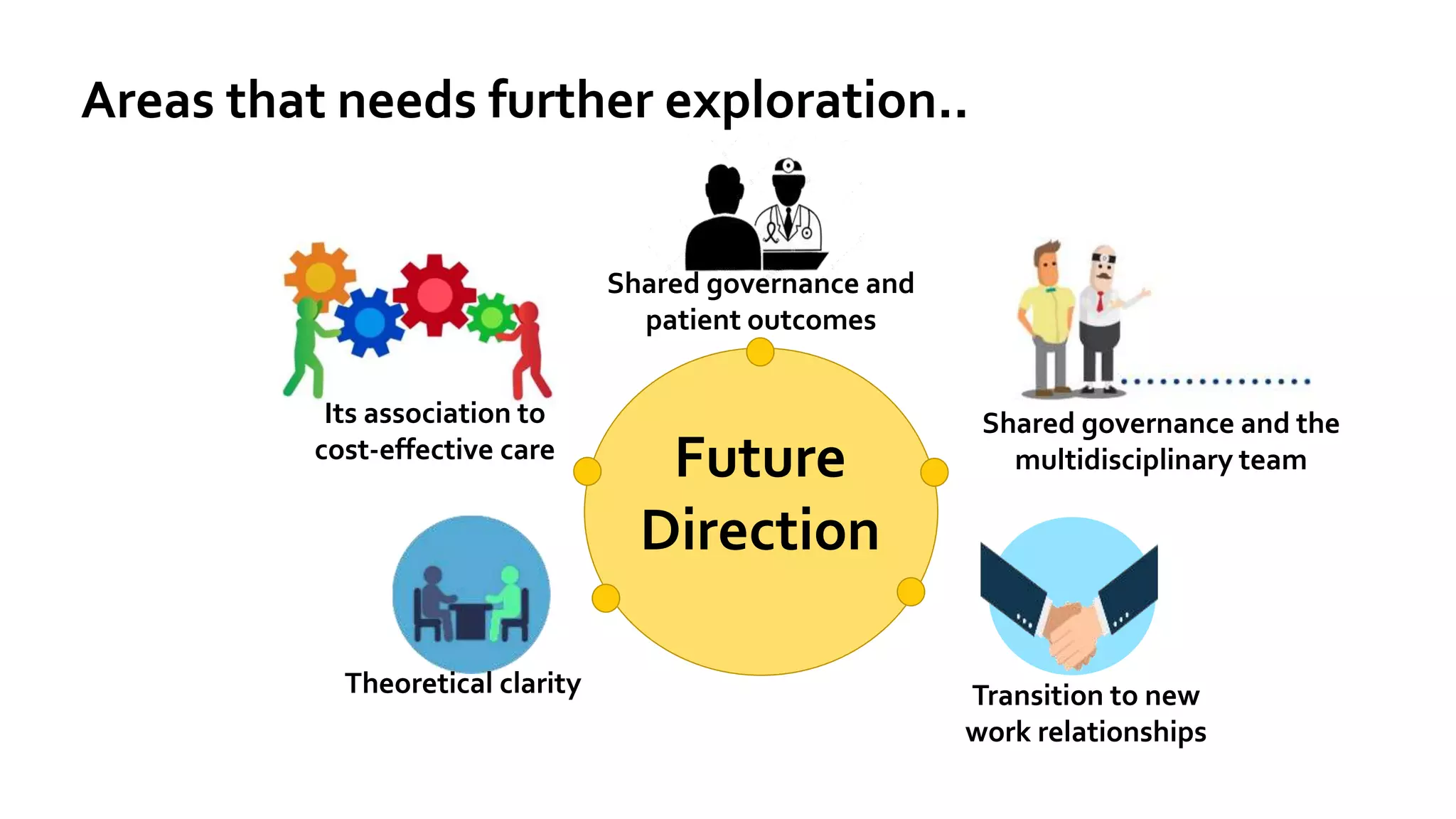
Theoretical clarity
Its associationto
cost-effective care
Shared governance and the
multidisciplinary team
Transition to new
work relationships
Shared governance and
patient outcomes
Future
Direction
Areas that needs further exploration..
22.
References:
Green, A. andJordan, C. (2004). Common Denominators: Shared
Governance and Work Place Advocacy-Strategies for Nurses to Gain Control
over Their Practice. The Online Journal of Issues in Nursing. Vol. 9 No.1,
Manuscript 6.
Guanci, G. (2018). Shared Governance: What it Is and Is Not. Association for
Nursing Professional Development. Retrieved from:
https://www.anpd.org/blog/shared-governance-what-it-is-and-is-not
Hess RG Jr. (2004). From bedside to boardroom - nursing shared
governance. Online J Issues Nurs. 9(1):2. Published 2004 Jan 31.
Anthony, M. (2004). "Shared Governance Models: The Theory, Practice, and
Evidence". Online Journal of Issues in Nursing. Vol. 9 No. 1, Manuscript 4.
Church, J., Baker, P., Berry, D. (2008). Shared governance: A journey with
continual mile markers. Nursing Management, 39 (8).
23.
References:
Porter-O'Grady, T. (2019)Principles for sustaining shared/professional governance
in nursing. Nursing Management (Springhouse).Vol 50 Issue 1 - p 36-41
McKnight H and Moore S. (2019) Nursing Shared Governance. In: StatPearls
StatPearls Publishing. Retrieved from:
https://www.ncbi.nlm.nih.gov/books/NBK549862/
O'May, Fiona & Buchan, James. (1999). Shared governance: A literature review.
International journal of nursing studies. 36. 281-300. 10.1016/S0020-
7489(99)00023-1.
24.
Quality efforts failbecause we lack “A”.
Enabler for Cultural Change
Q x
Quality solutions x
= EA
Formula for Success….
= Effective ResultsAcceptance and Accountability
Shared Governance is a journey, not a destination.
25.
These slides areuploaded for information purposes and as partial
requirement of Philippine Womens’ University in PhD Class;
Subject: Governance in Healthcare Practice with
Dr. David Hali de Jesus, RN, PgDip, FISQua
Editor's Notes
#5 In developed countries, acute respiratory tract infections account for 20% of all medical consultations and 75% of all antibiotic prescriptions causing economic burden. URTI is mostly recurrent in children that may lead to a decline in lung function resulting to multiple medical visits and frequent school absenteeism. In PEC, not all URTI’s are being prescribed with antibiotics as presented in the case of the 2-year old child as it may only lead to antibiotic overdose and bacterial resistance as well. These findings suggest that early optimal treatment is beneficial to the recovery of quality of life.
#8 In the past decades, since 1912, it was discovered that MgSO4 has a bronchodilatory property but research still continues because the exact mechanism of how MgSO4 benefits patients experiencing asthma exacerbations is still largely restricted.
#12 Vitamin D status is determined by measuring level of serum 25-hydroxyvitamin D 25-(OH)D, which is the active form
The endocrine society defined deficiency as 25-hydroxy vitamin D of ≤ 20 ng/ml, Insufficiency as level of 21-29ng/ml, an individual with 30 -100ng/ml of 25hydroxyvitamin D as sufficient.
The Endocrine society further recommends screening of Vitamin D for individual at risk.
#20 To bring things to a close, well with all the recommendations, policies, guidelines & supporting evidences I conclude we have reached the objective of this talk & cleared the roadblocks and increased our awareness & the appropriate use of oseltamivir treatment.
Let us bear in mind as well the trade-off between benefits and harms when making decisions to use oseltamivir for treatment, prophylaxis, or stockpiling.