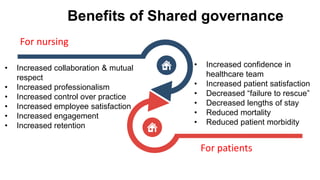
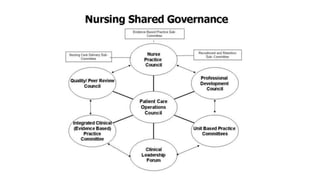
Shared governance is a model of nursing leadership that promotes participatory decision making between nurses and administration. It aims to empower nurses and give them more control over their practice. There are four key principles: partnership, equity, accountability, and ownership. Shared governance can be implemented through various council models and provides benefits like increased job satisfaction and patient outcomes. However, obstacles like resistance to change must be overcome through strategies like strong nurse leadership, education, and clear communication.