Downloaded 637 times

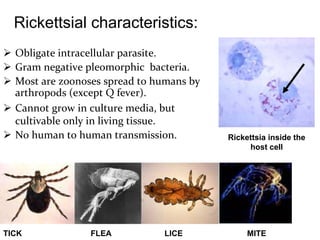
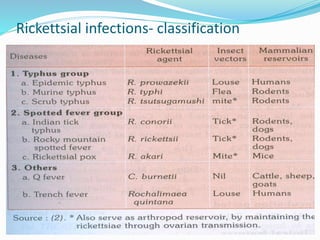
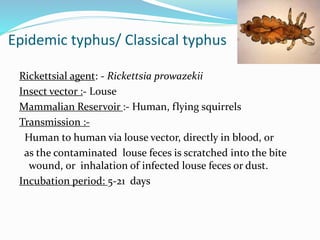




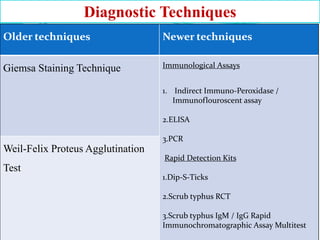


Rickettsial diseases are difficult to diagnose clinically and often go unrecognized, leading to significant morbidity and mortality. They are caused by intracellular bacteria from the Rickettsia genus that are typically spread by arthropod vectors like ticks, fleas and mites. Some of the most common rickettsial diseases found in India include scrub typhus, murine typhus, Indian tick typhus and Q fever. Diagnosis relies on clinical suspicion combined with serology. Treatment involves doxycycline. Prevention focuses on vector control and improving hygiene.










































































