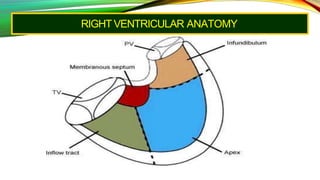
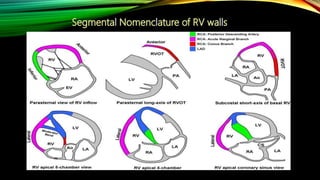
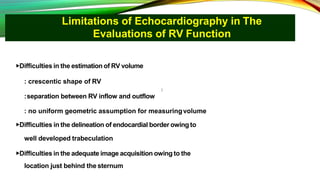
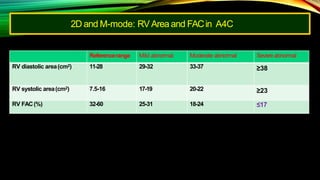
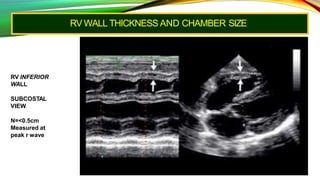
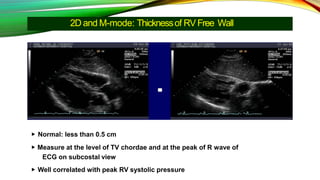
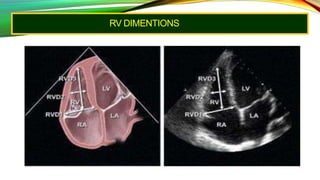
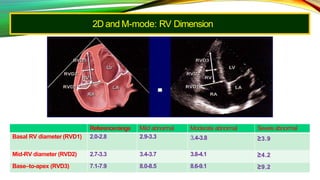
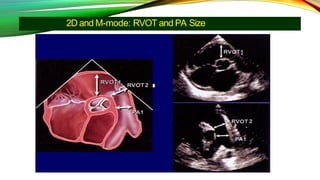
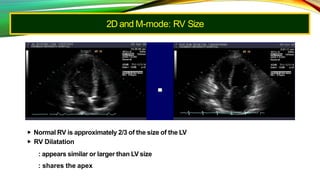
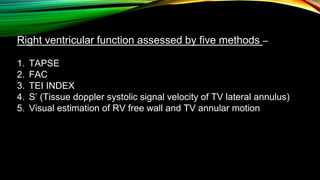
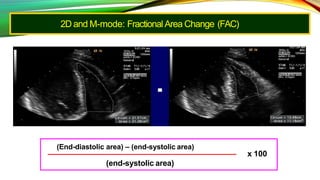
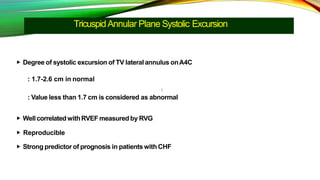
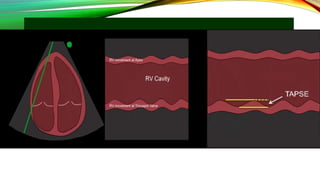
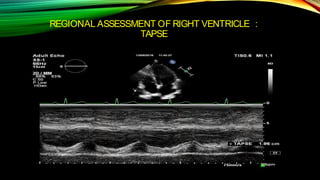
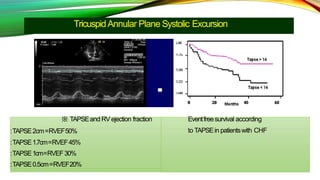
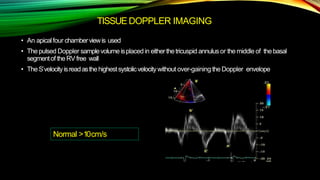
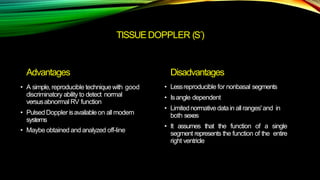
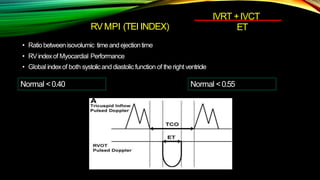
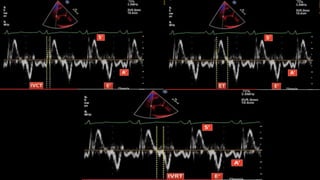
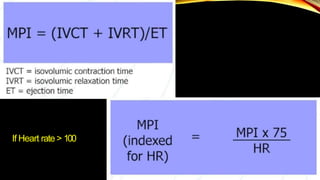
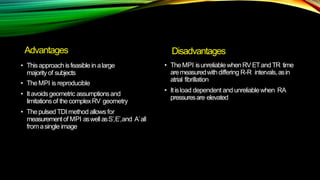
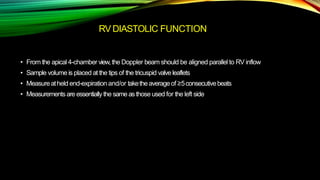
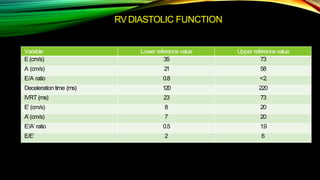
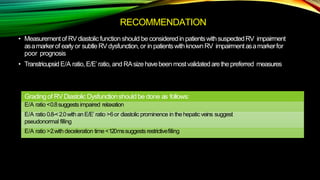
This document discusses the limitations and techniques for assessing right ventricular (RV) function using echocardiography. It is difficult to accurately evaluate RV volume, delineate borders, and image the entire RV using echocardiography due to its complex crescent shape. However, the document recommends using RV fractional area change, tricuspid annular plane systolic excursion, tissue Doppler S' velocity, and Tei index to quantitatively assess RV systolic function as they are reproducible methods. RV dimensions, wall thickness, and outflow tract size can also provide information on RV size and function. Assessment of RV diastolic function includes parameters like E/A ratio, E/E' ratio, and deceleration time.