Downloaded 5,051 times








Snake bites are a major public health issue in India, with estimates of 200,000 bites and 15,000-20,000 deaths annually. The document discusses the epidemiology, types of venomous snakes, clinical effects of envenomation, and management of snake bites. Management involves first aid measures like immobilization of the bite area, administration of antivenom serum, and supportive care. Antivenom serum is most effective when given within 4 hours of the bite to neutralize the venom, and mechanical ventilation may be needed if respiratory failure occurs from neurotoxic or systemic effects of the venom.
Introduction to snake bite envenomation by Dr. Vikas Kesarwani, Pulmonary & Critical Care Expert.
India witnesses 200,000 snake bites and 15-20,000 deaths annually, with a 2:1 male-to-female ratio and most bites on lower limbs.
India witnesses 200,000 snake bites and 15-20,000 deaths annually, with a 2:1 male-to-female ratio and most bites on lower limbs.
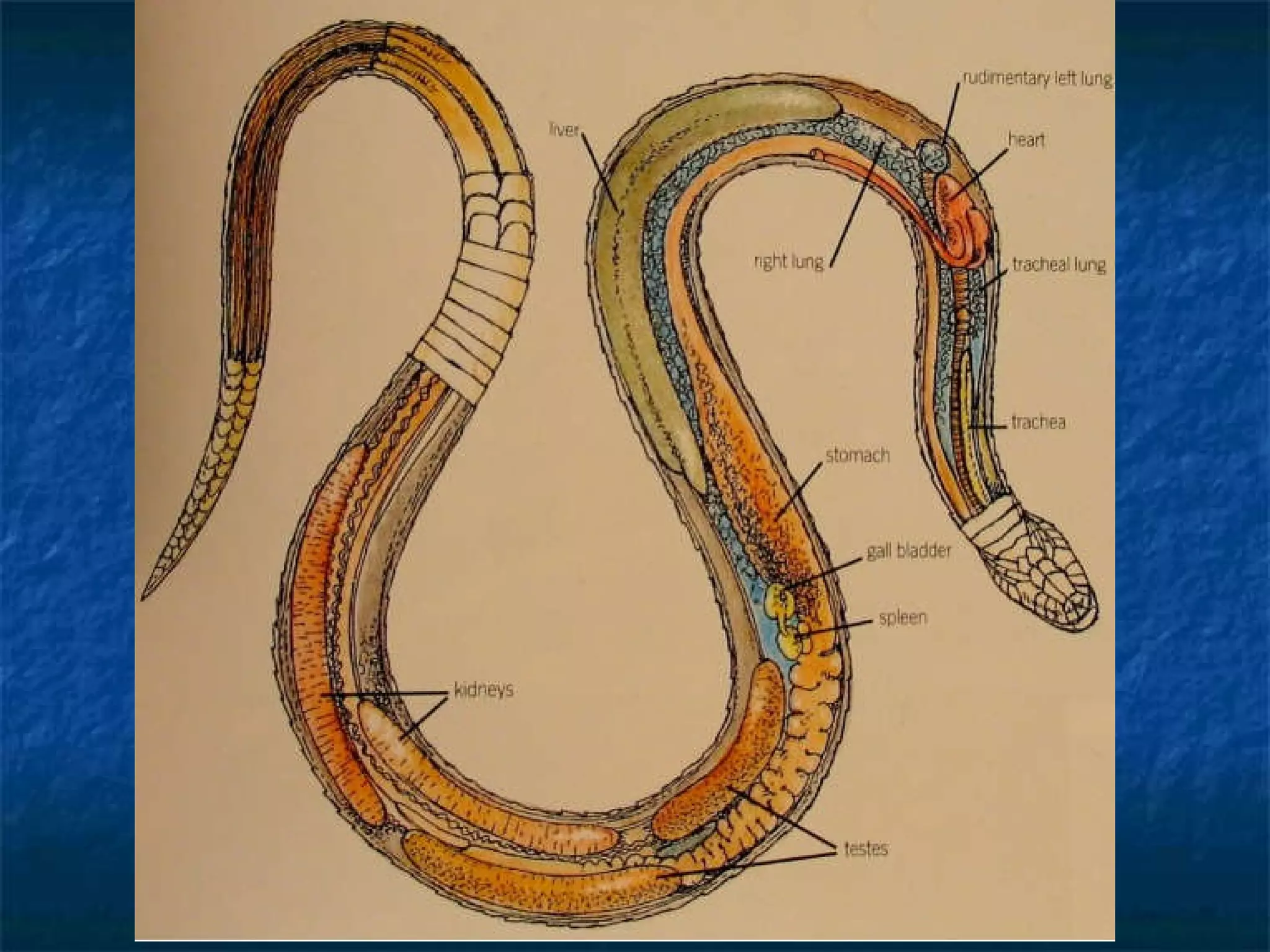
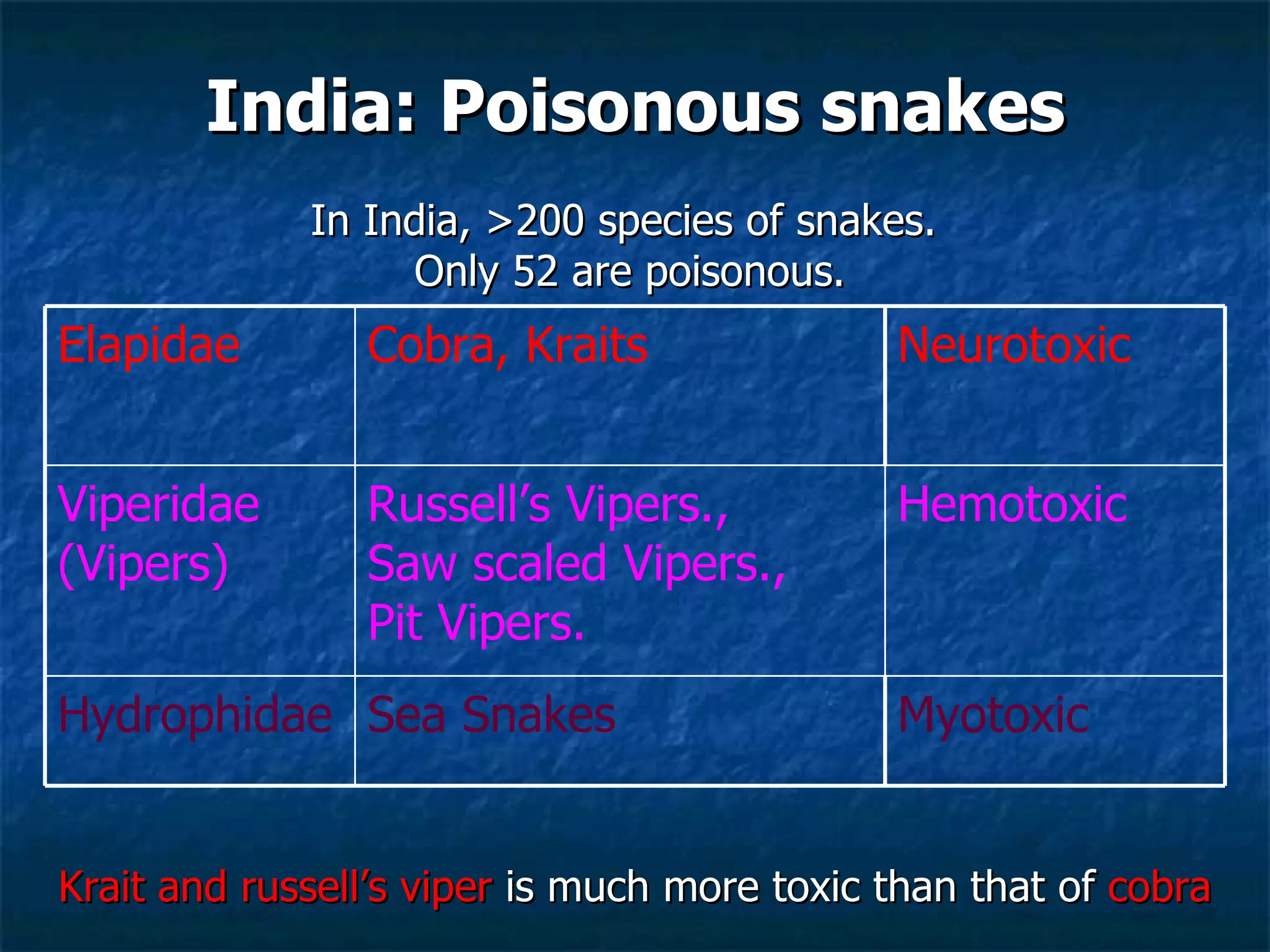
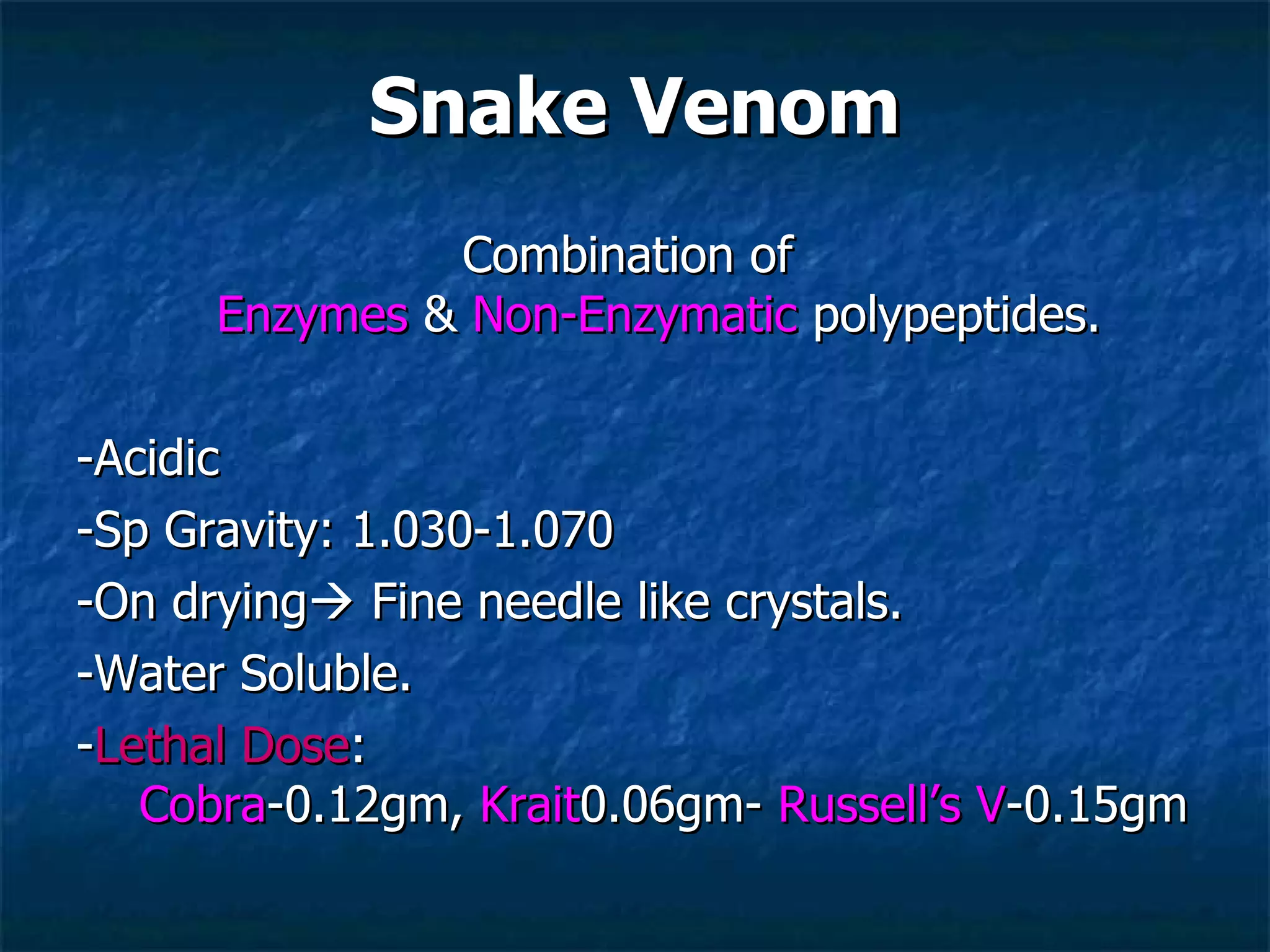
Introduction to snake anatomy, thermoregulation, types of venomous snakes in India, and venom characteristics including lethal doses.
Introduction to snake anatomy, thermoregulation, types of venomous snakes in India, and venom characteristics including lethal doses.
Introduction to snake anatomy, thermoregulation, types of venomous snakes in India, and venom characteristics including lethal doses.
Diagnosis based on fang marks, varying from 8mm to 4cm apart, indicating species of snake.
Local and systemic effects of venomous bites classified by snake types (Elapid, Viperid, Hydrophid) with specific symptoms.
Management strategies including local measures such as pressure and ASV, which is critical in treatment.
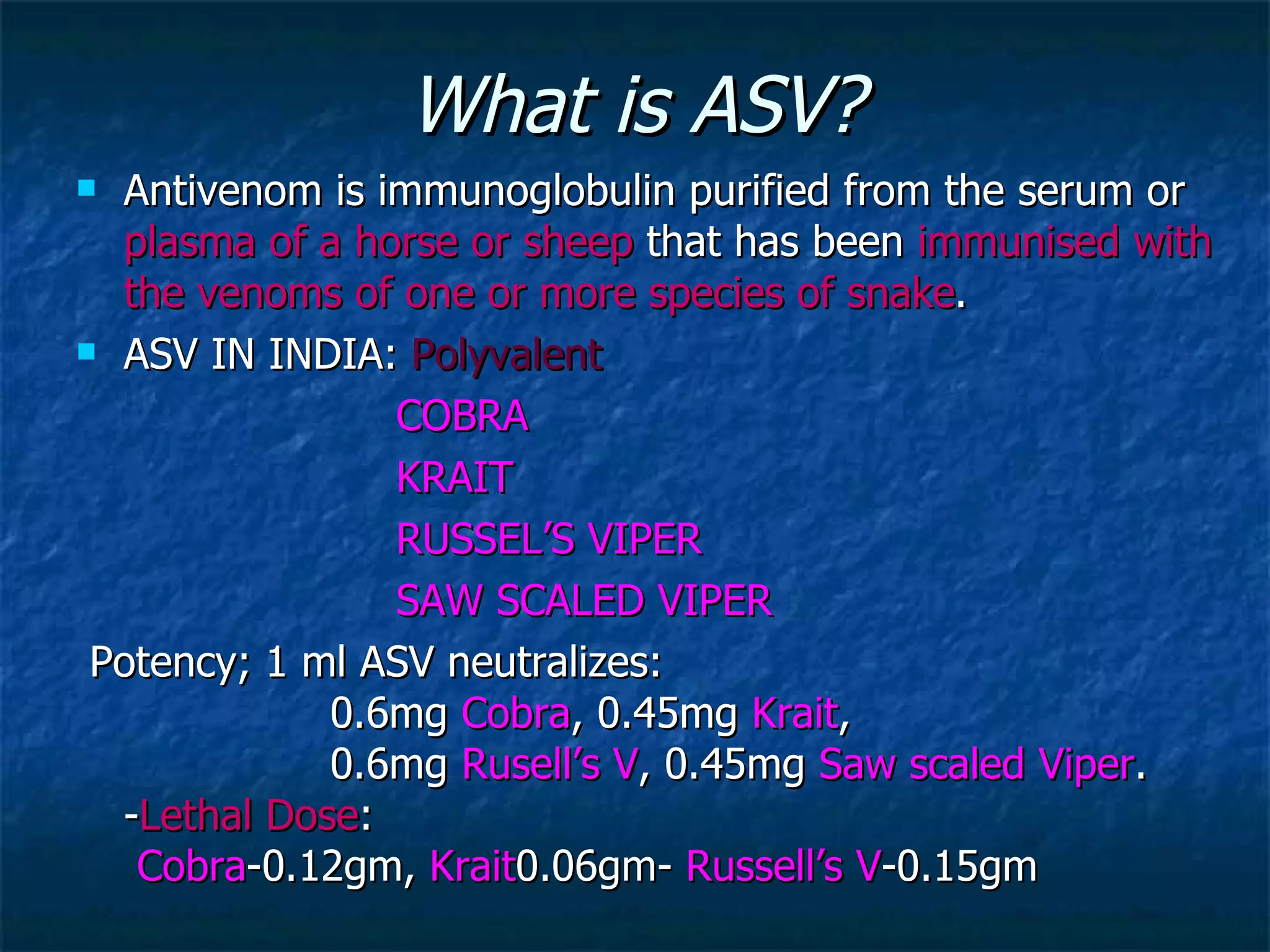
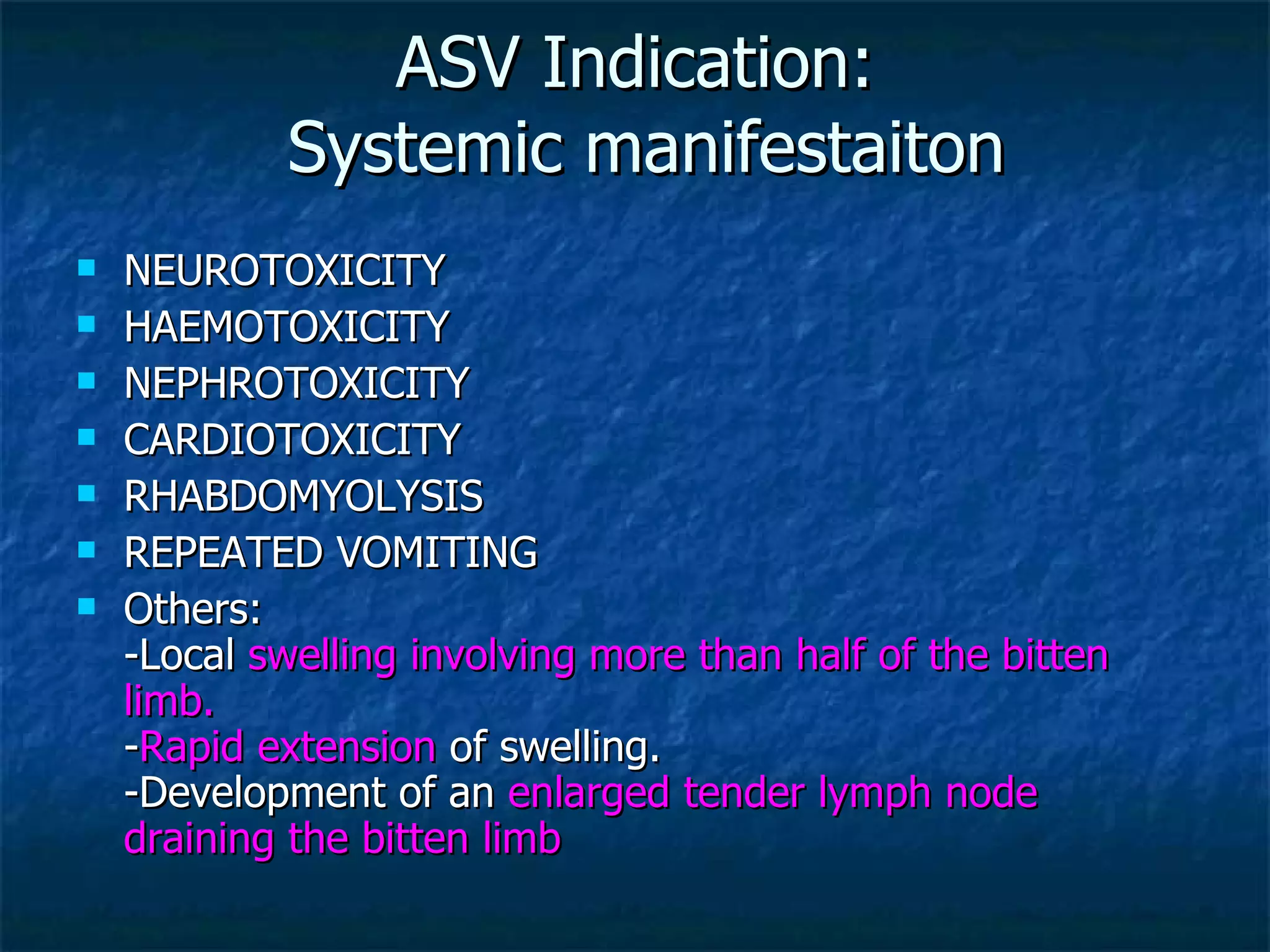
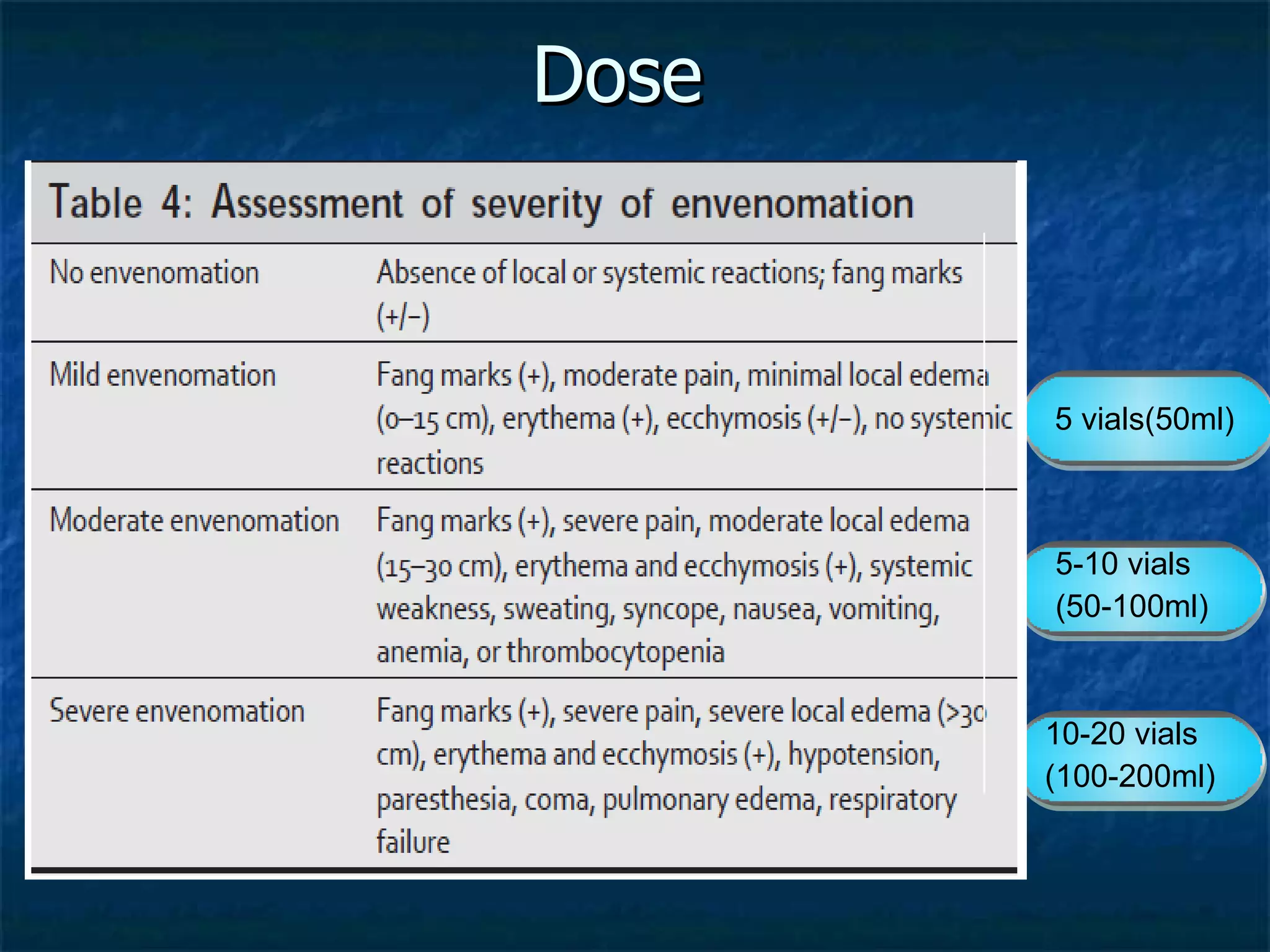
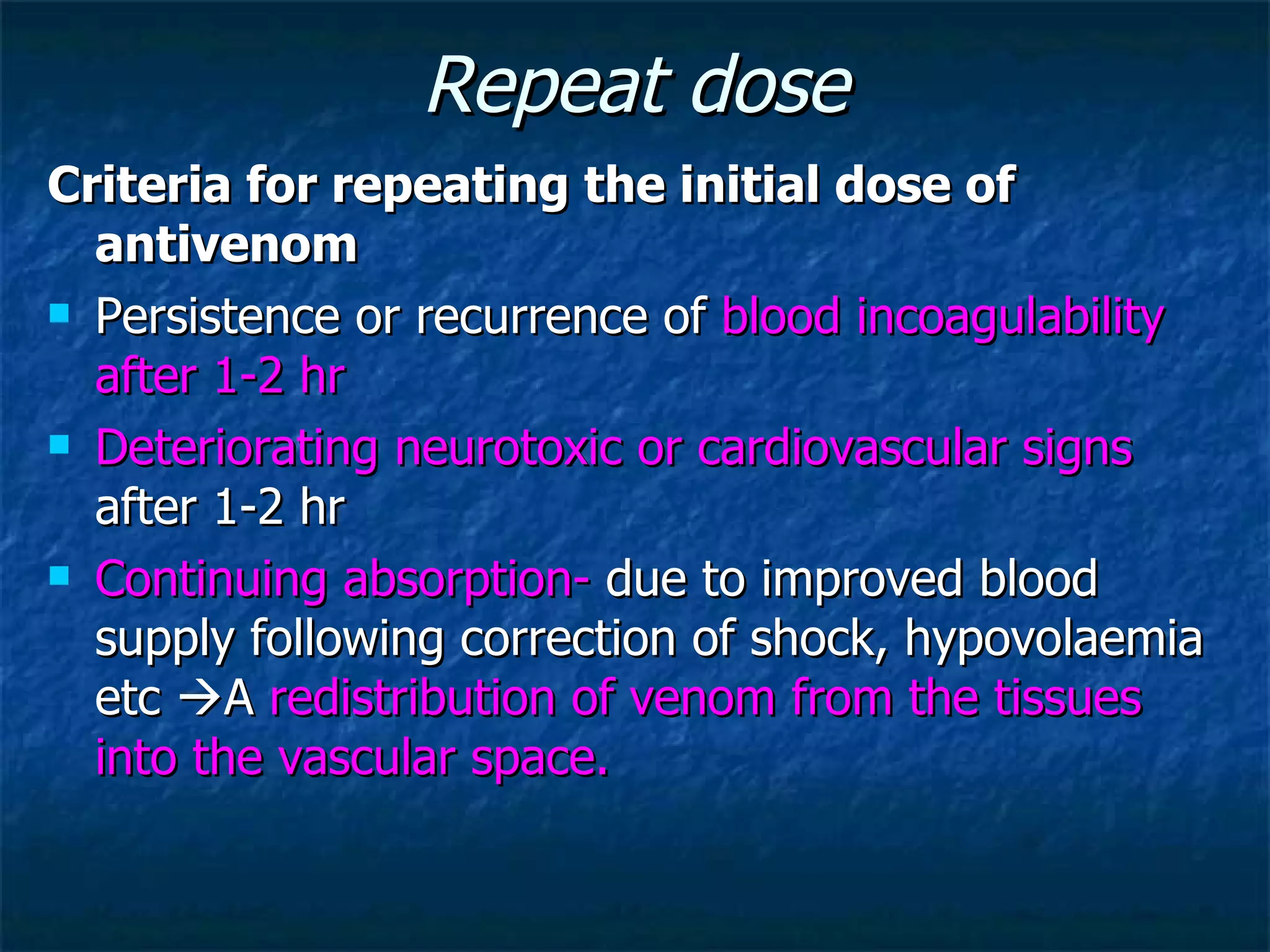
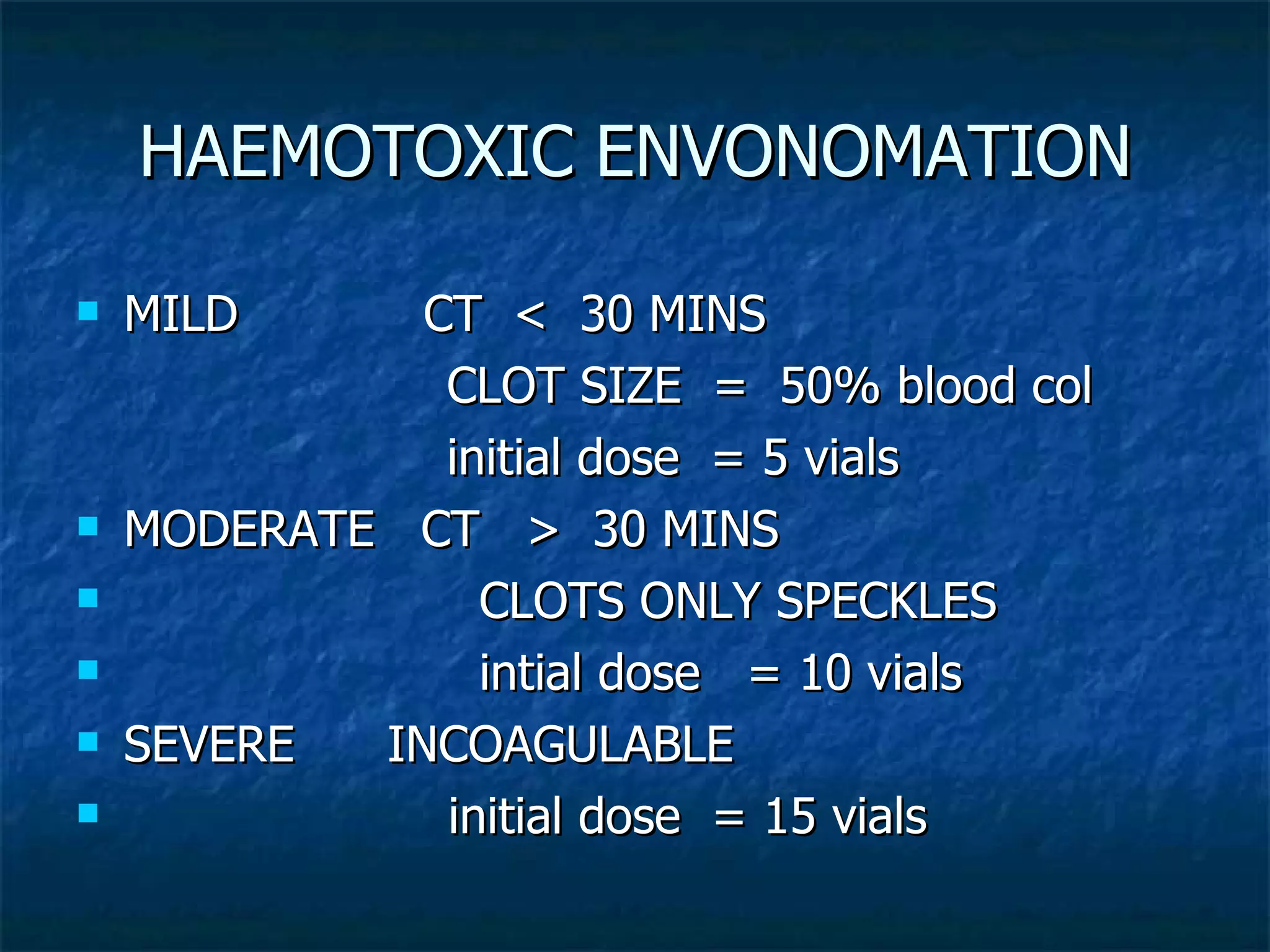
Details on ASV's effectiveness, dosing protocols, potential reactions, and management options for children.
Supportive care recommendations including IV fluids, airway management, and a summary of ASV necessity based on clinical features.
Supportive care recommendations including IV fluids, airway management, and a summary of ASV necessity based on clinical features.












































































