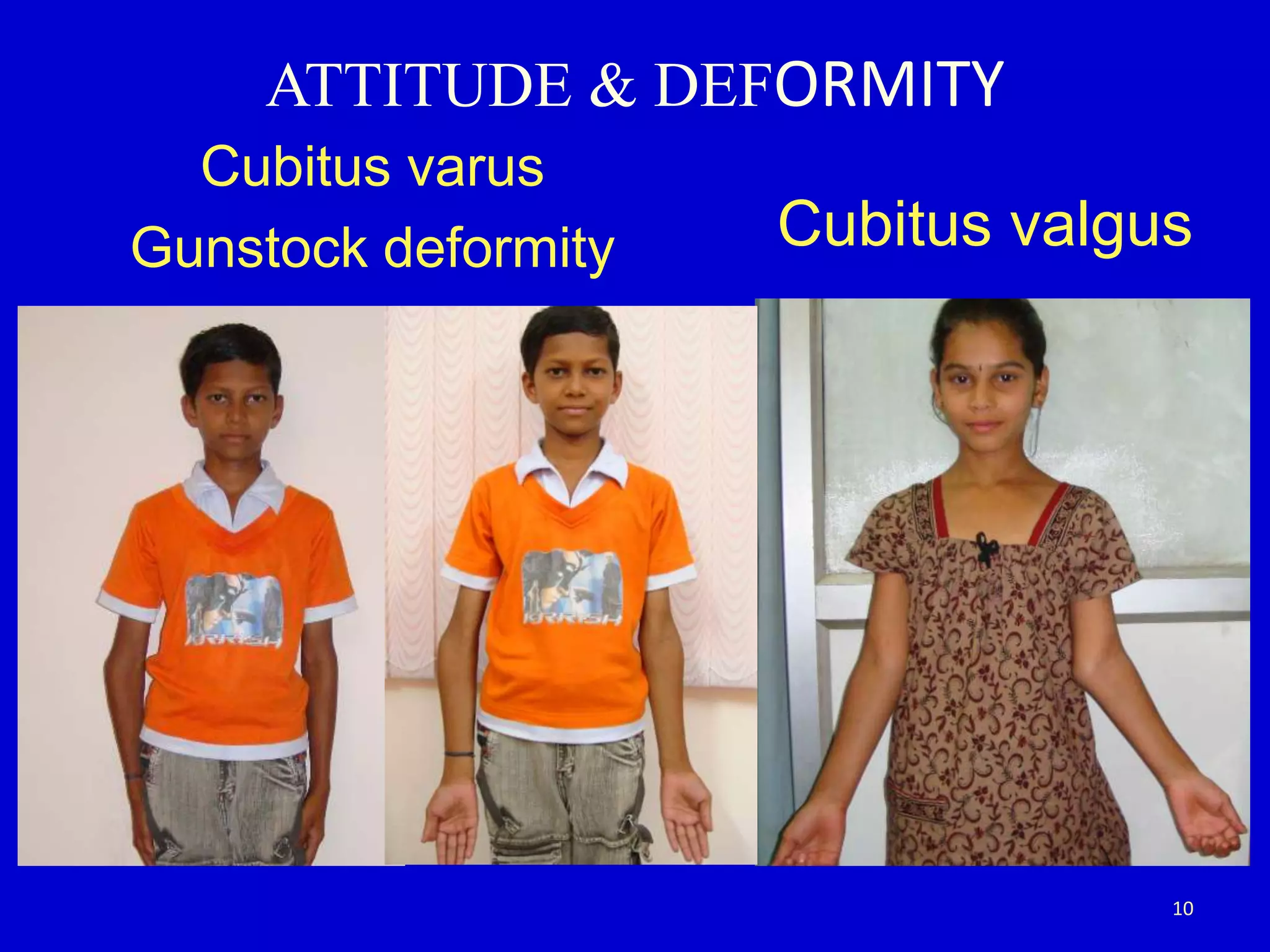
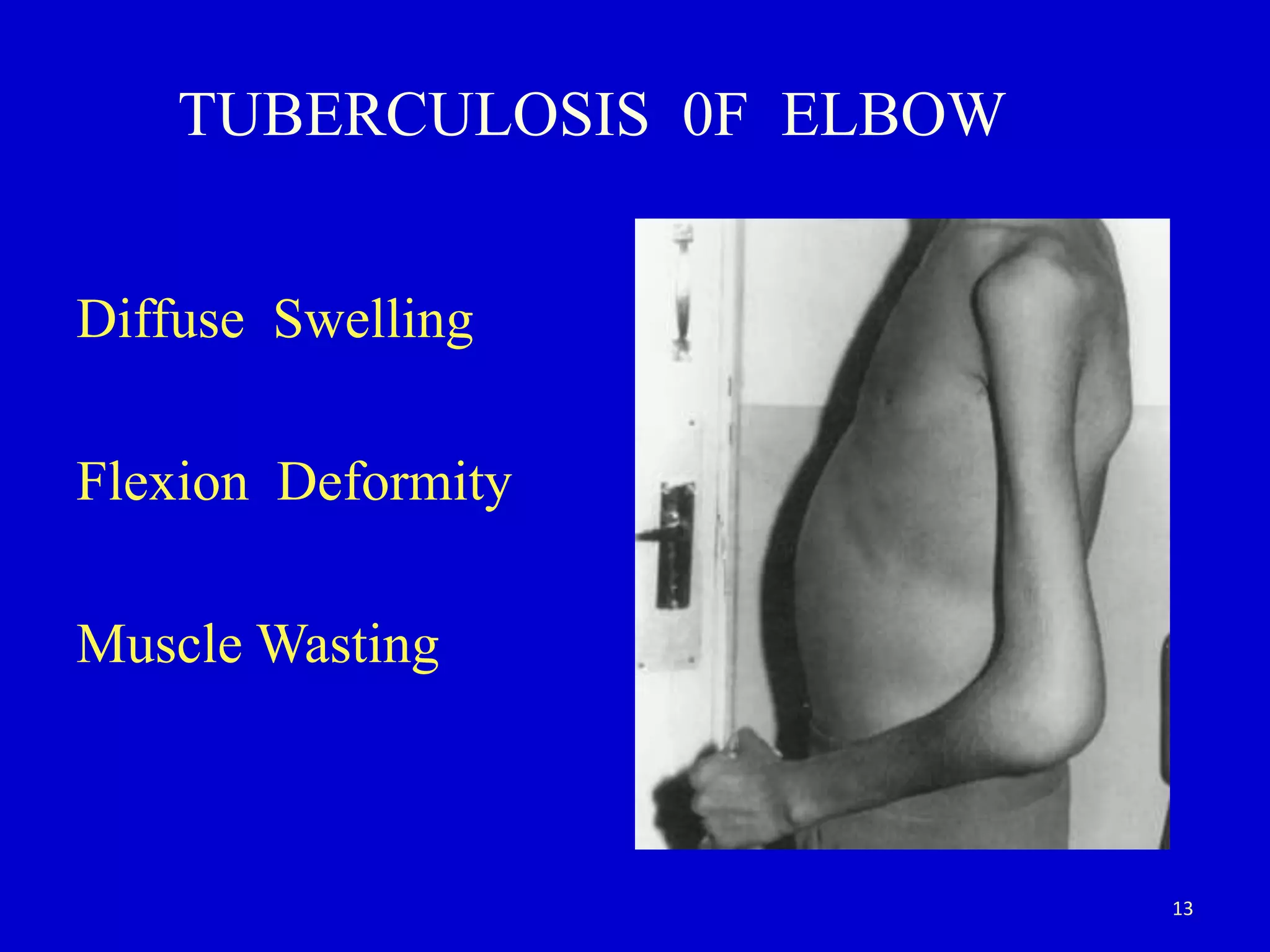
This document provides guidance on clinical examination of the elbow joint. It describes the different approaches needed for traumatic versus non-traumatic conditions, as well as acute versus chronic injuries. The elbow is examined through inspection, palpation, range of motion testing, and special tests. Common injuries like tennis elbow, pulled elbow in children, and fractures are discussed. Key examination findings for conditions like cubitus varus, cubitus valgus, and myositis ossificans are also outlined.