Downloaded 82 times


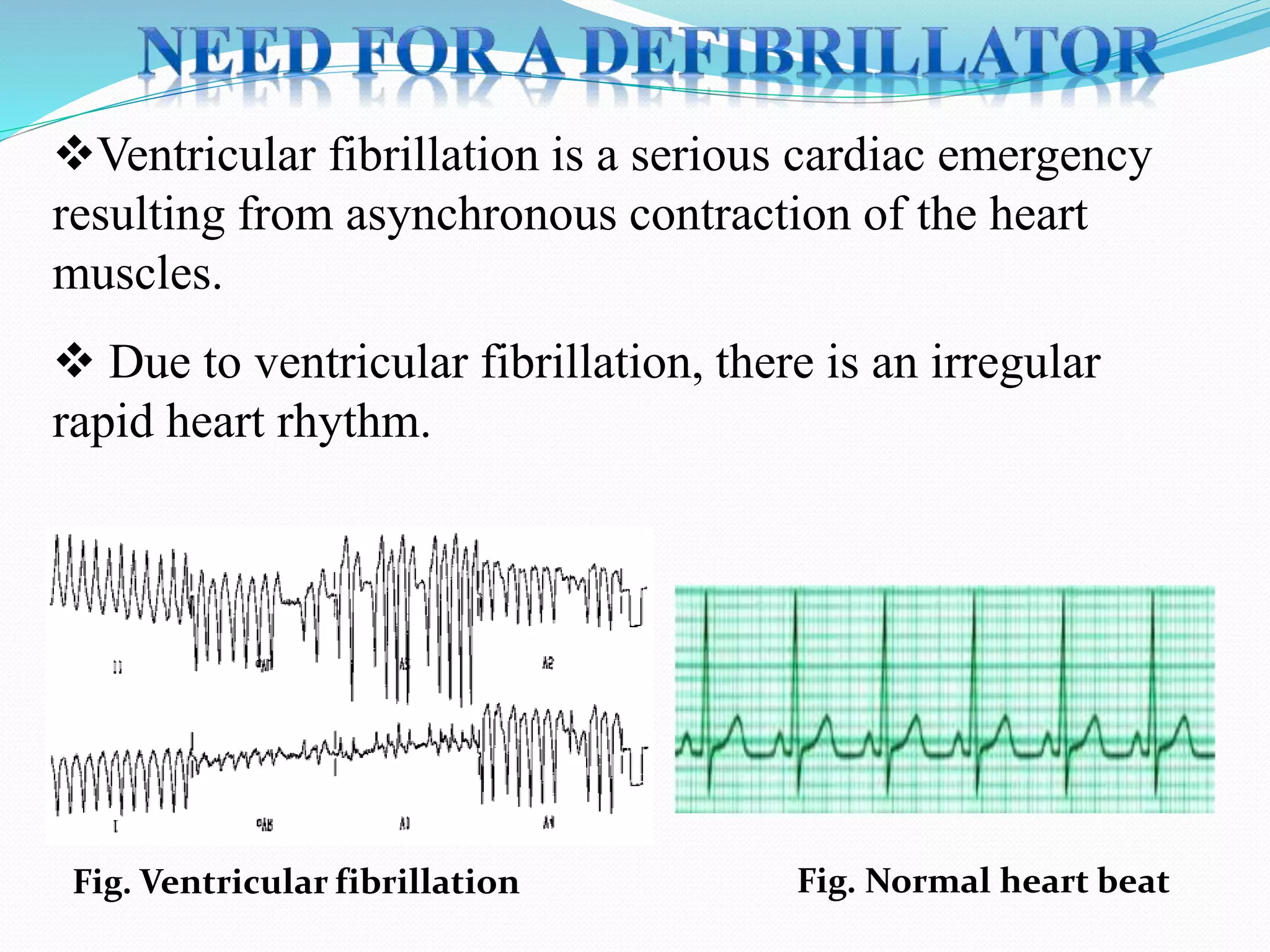
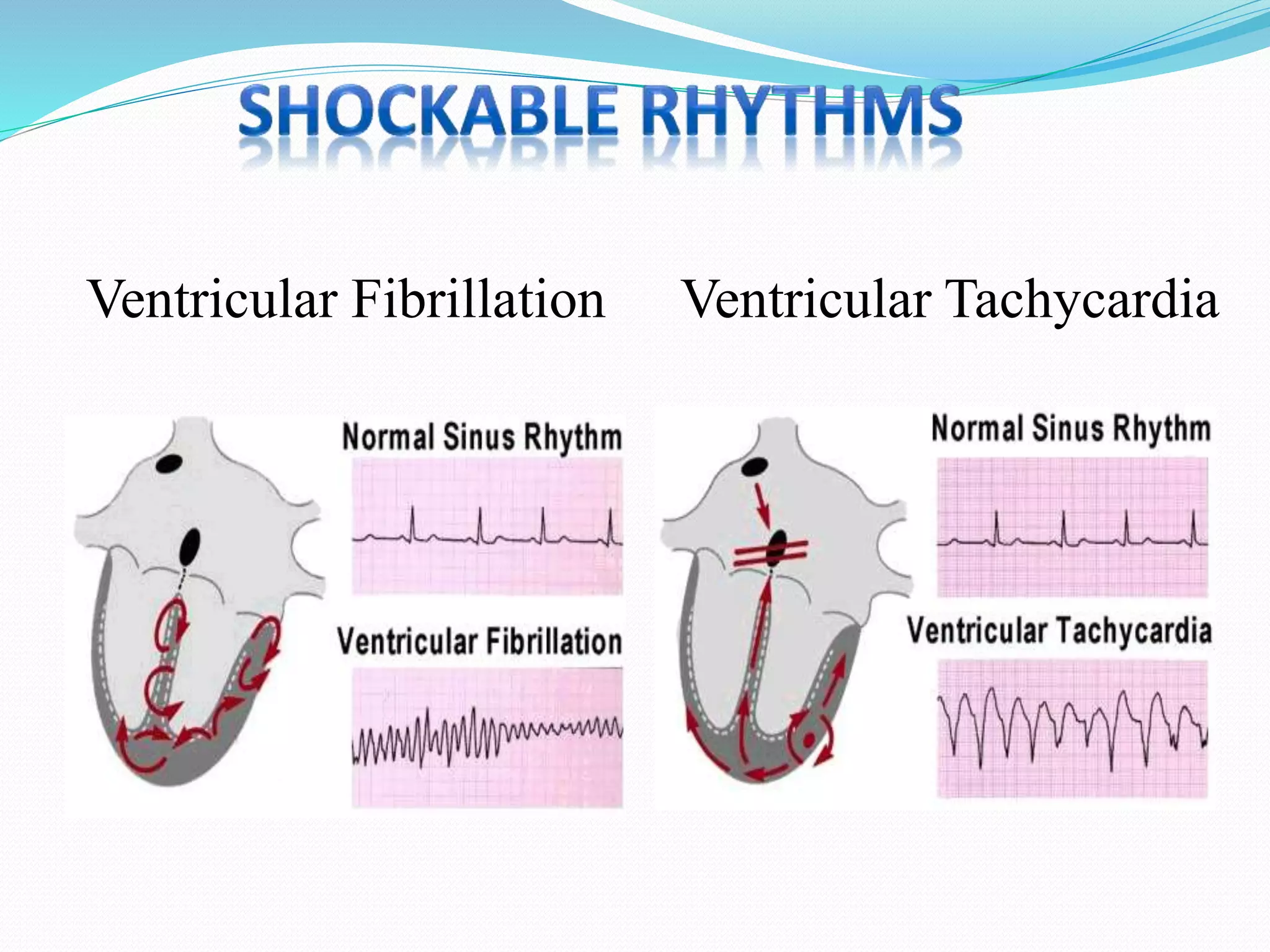
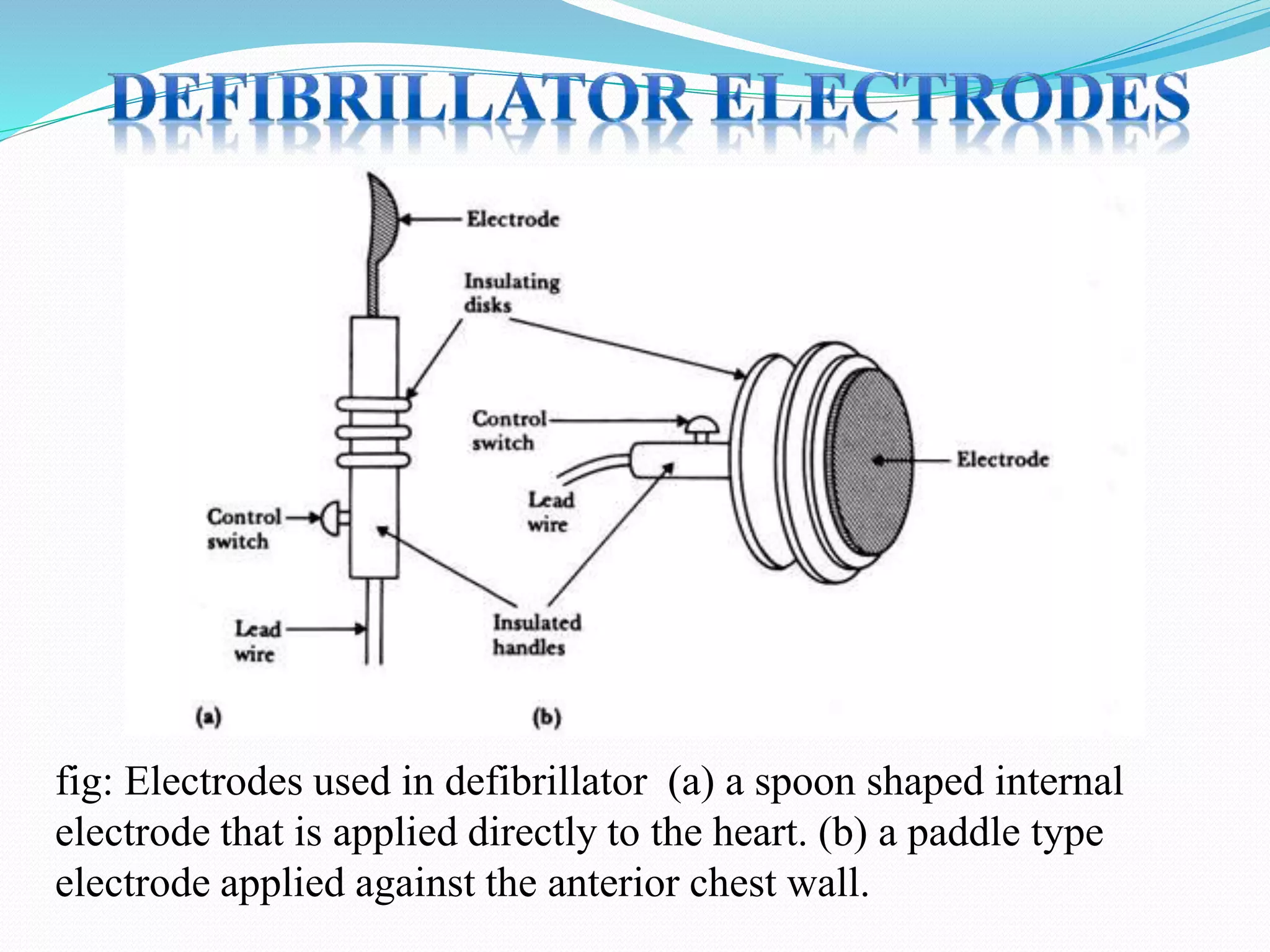

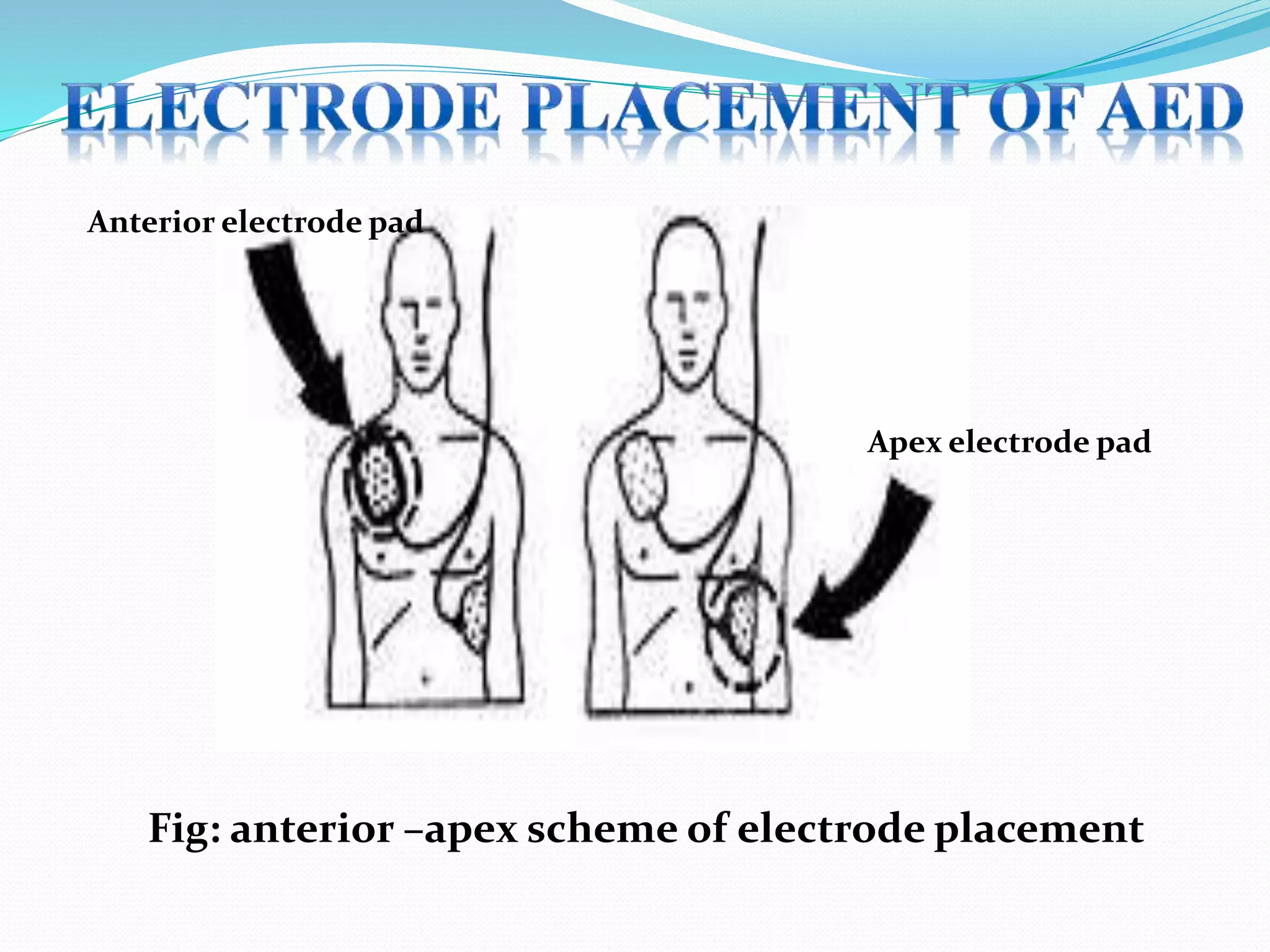
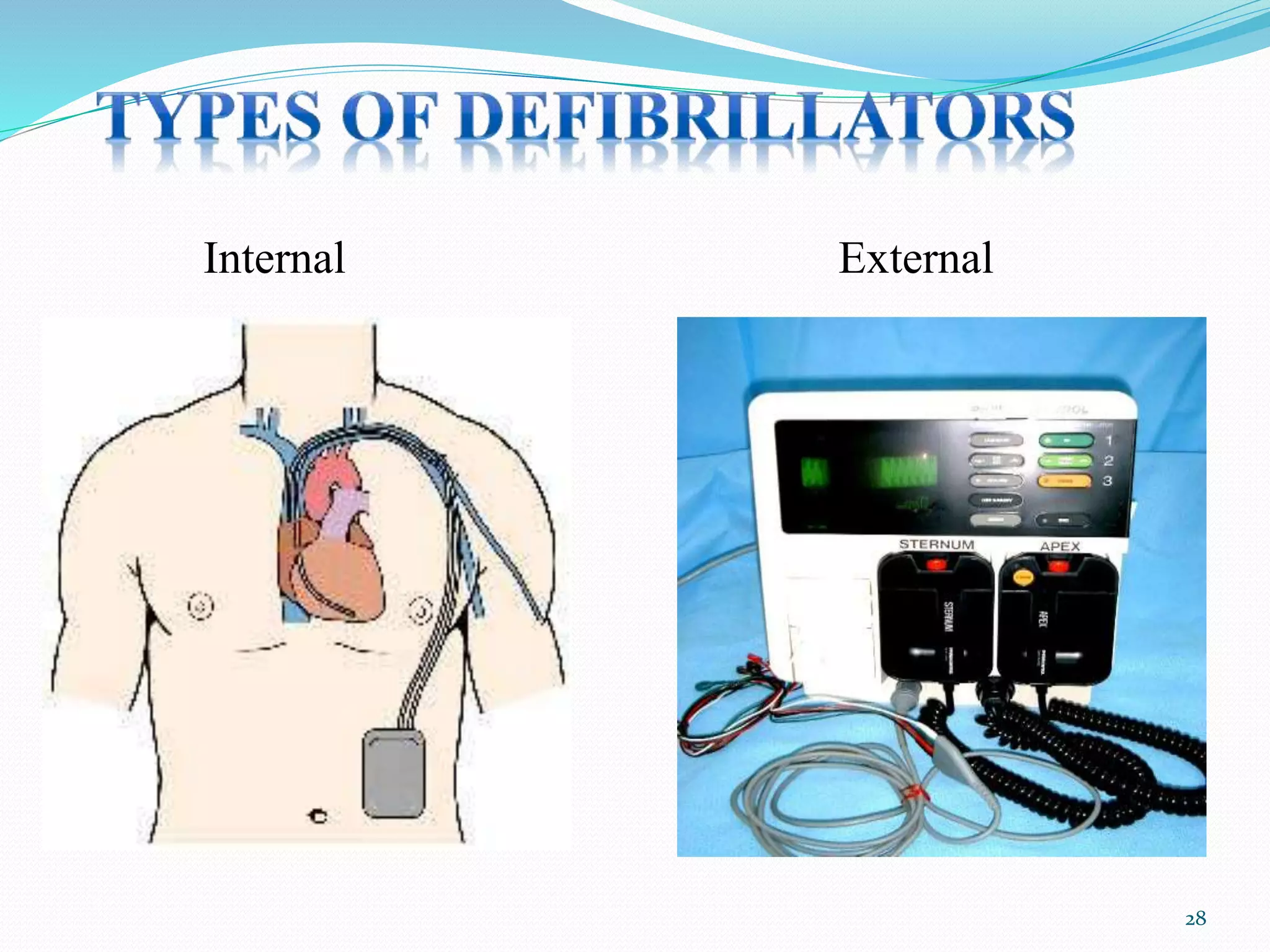


Defibrillation is a process that delivers an electric shock to the heart to stop ventricular fibrillation and restore normal rhythm. It involves using a defibrillator to detect and correct dangerous heart rhythms. There are external defibrillators like AEDs that can be used by laypeople, as well as internal defibrillators implanted in the body. The shock delivered must be of sufficient energy to depolarize enough heart muscle to terminate fibrillation. Proper use and troubleshooting of defibrillators is important for reviving someone experiencing cardiac arrest.













































































