Downloaded 407 times




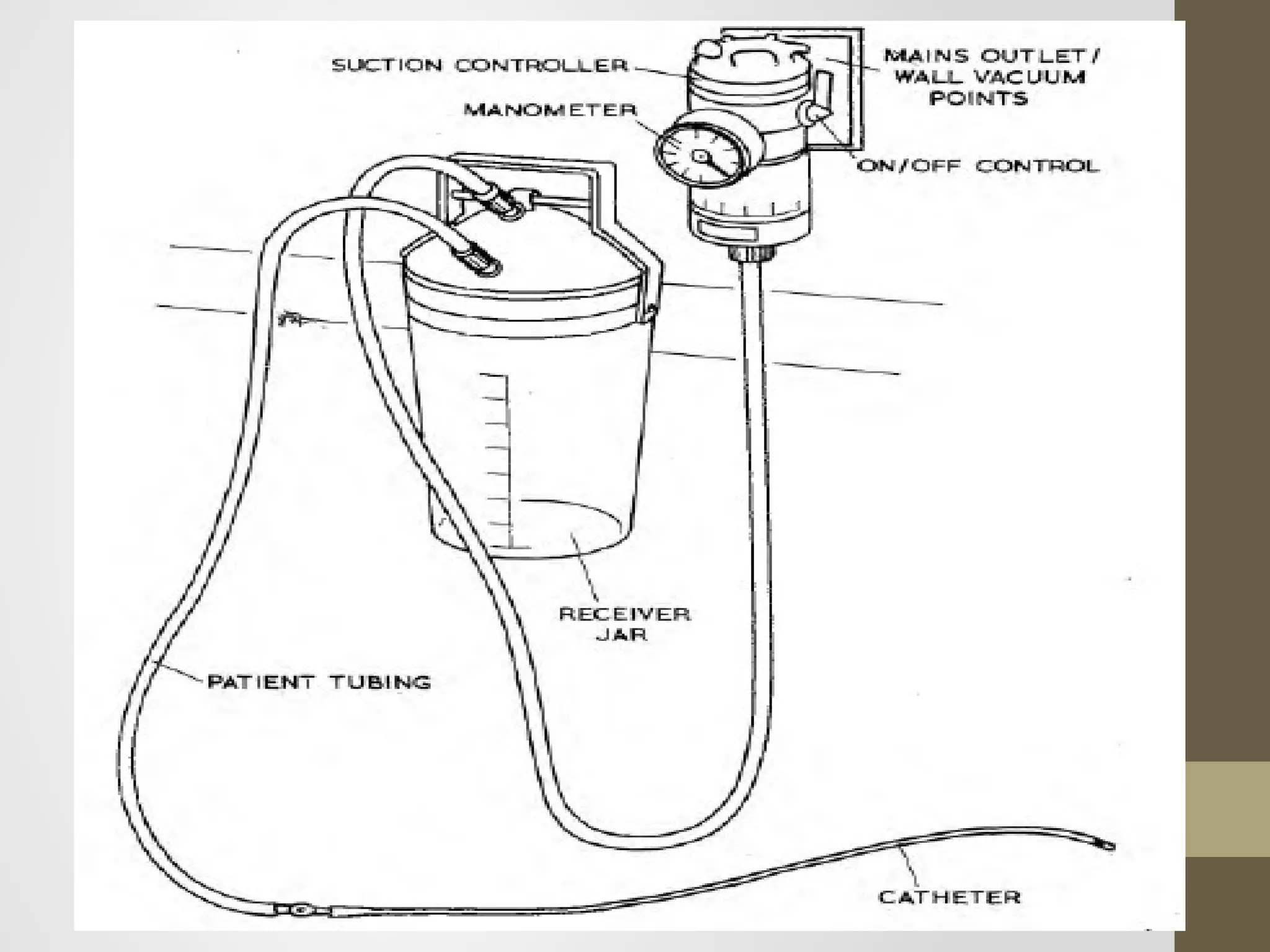

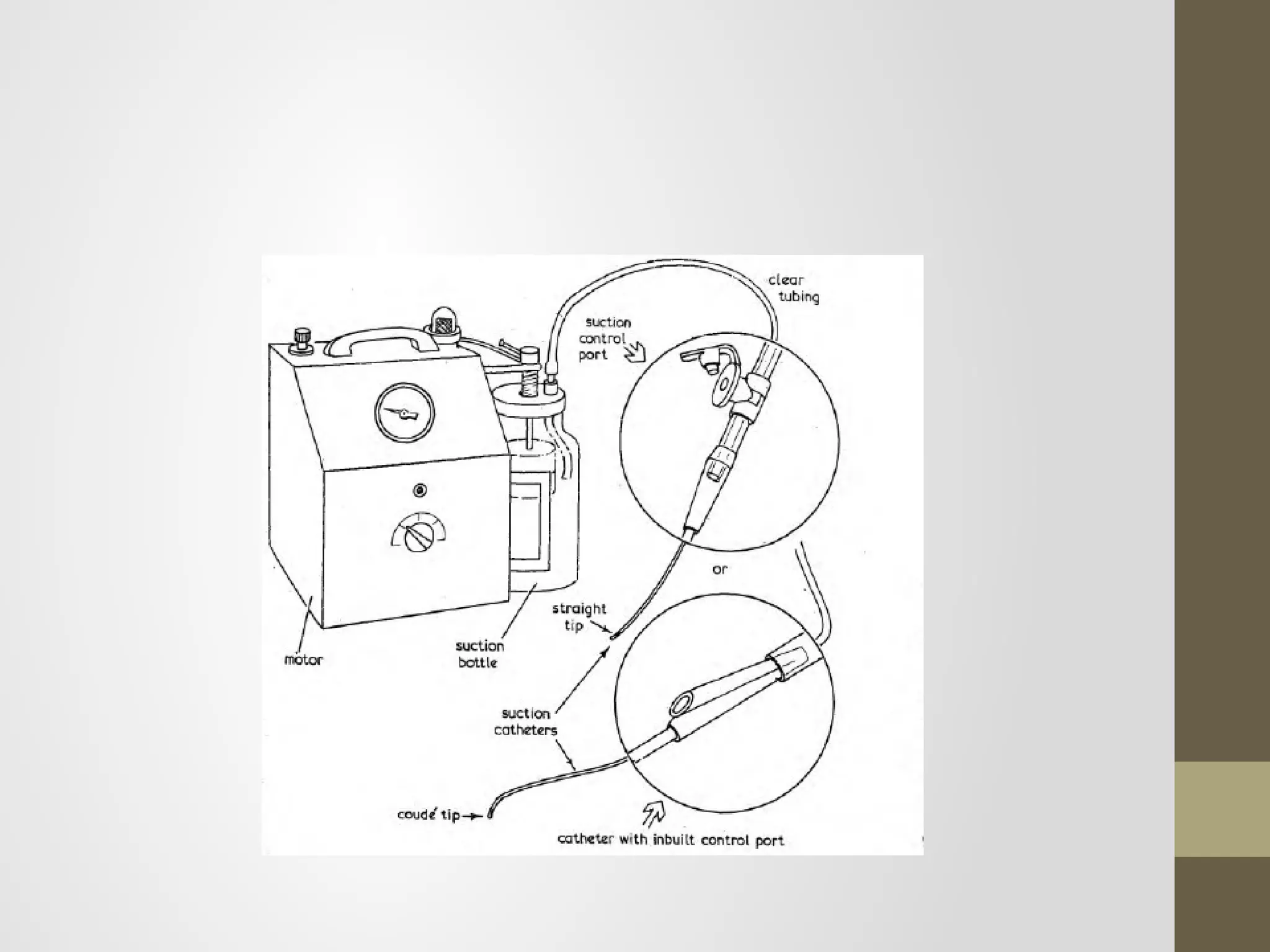












Suction is frequently used to remove secretions from the lungs in intubated or tracheostomy patients unable to cough effectively. Proper suction equipment includes pumps, tubing, connections, and catheters. Pumps can be wall vacuum, electrical, portable battery-powered, or foot pumps. Tubing leads from pumps to connections, usually Y-connectors. Catheters come in soft plastic or rubber and range in size but should not exceed half the tube diameter. Proper suction technique minimizes trauma and hypoxia through controlled pressure and timing.
Overview of airway suction usage for secretion removal in intubated patients.
Discusses types of suction equipment including pumps, tubing, connections, and catheters.Different catheters' characteristics including sizes, types, and specialized uses.
Essential items for a suction trolley, including gloves, catheters, and sterilization tools.
Various suction techniques, their execution, and precautions to minimize complications.























































































