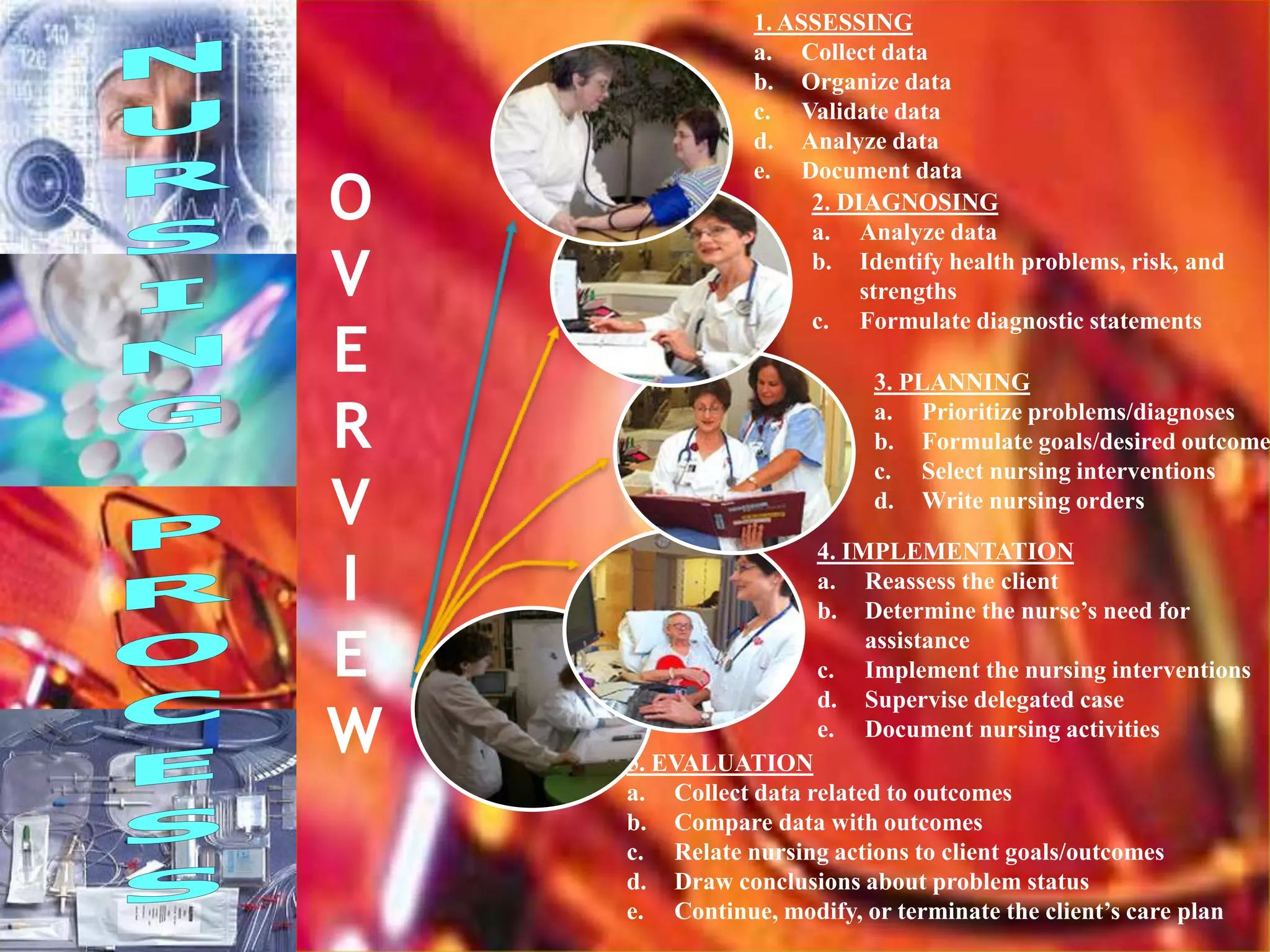
1. The nursing process is a systematic, rational method of planning and providing individualized nursing care.
2. It involves assessing a client's health status, planning care based on the assessment, implementing interventions, and evaluating the outcomes of care.
3. The nursing process allows nurses to identify health problems, establish goals, and deliver specific interventions to meet client needs.


![4. Characteristics of the Nursing
Process
1] Cyclic & dynamic in nature
2] Client centered
3] Focus on problem solving & Decision making
4] Interpersonal & Collaborative style
5] Universal applicability
6] Use of critical thinking.
7] Data from each phase provide input into the next
phase.
8]Decision making involved in every phase of nursing
process.](https://image.slidesharecdn.com/nursingprocess-assessing-111105015609-phpapp01/75/Nursing-process-assessing-15-2048.jpg)
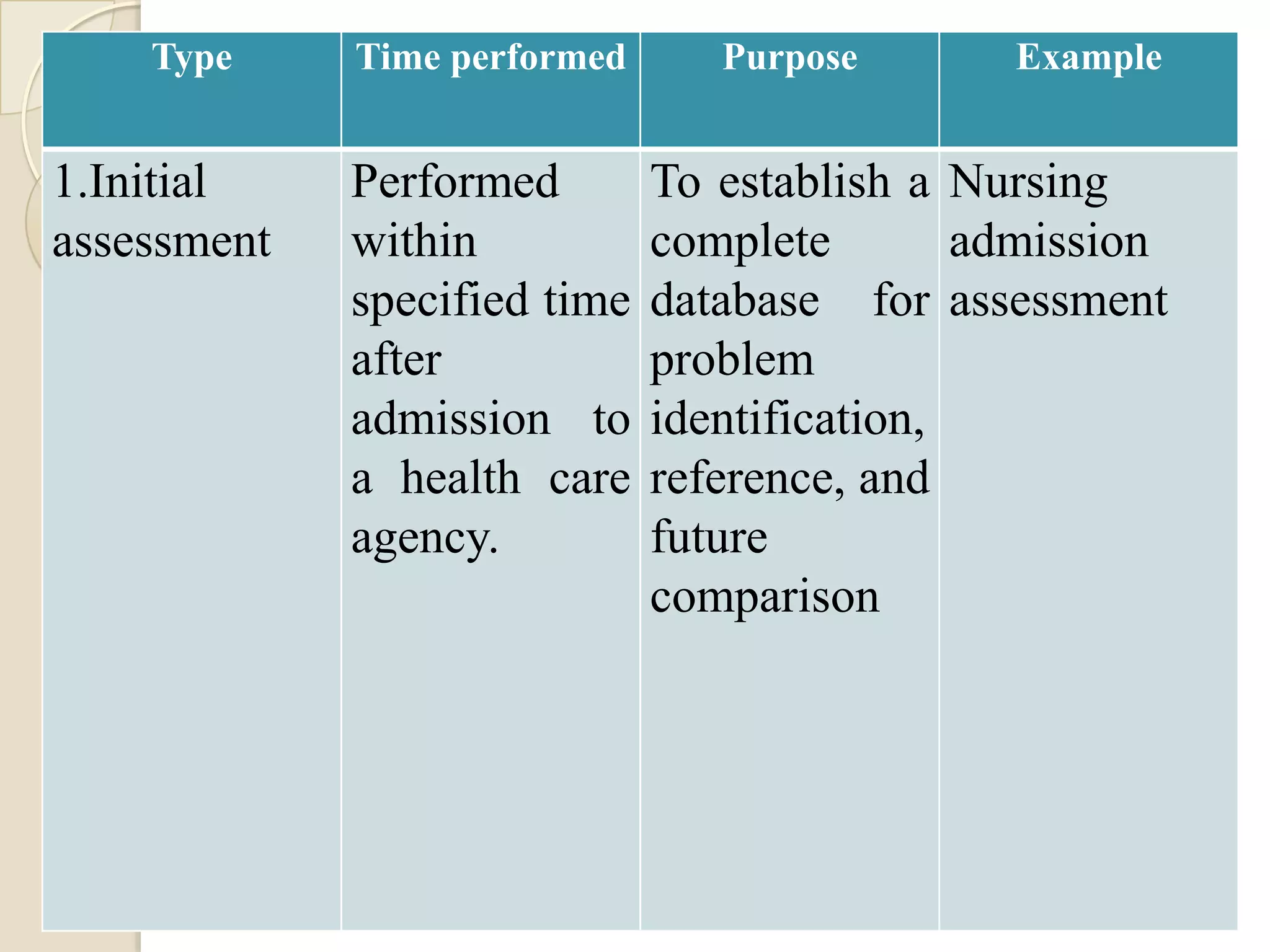
![5. c. Types of assessment
There are 4 different types of
assessment:-
1] Initial assessment
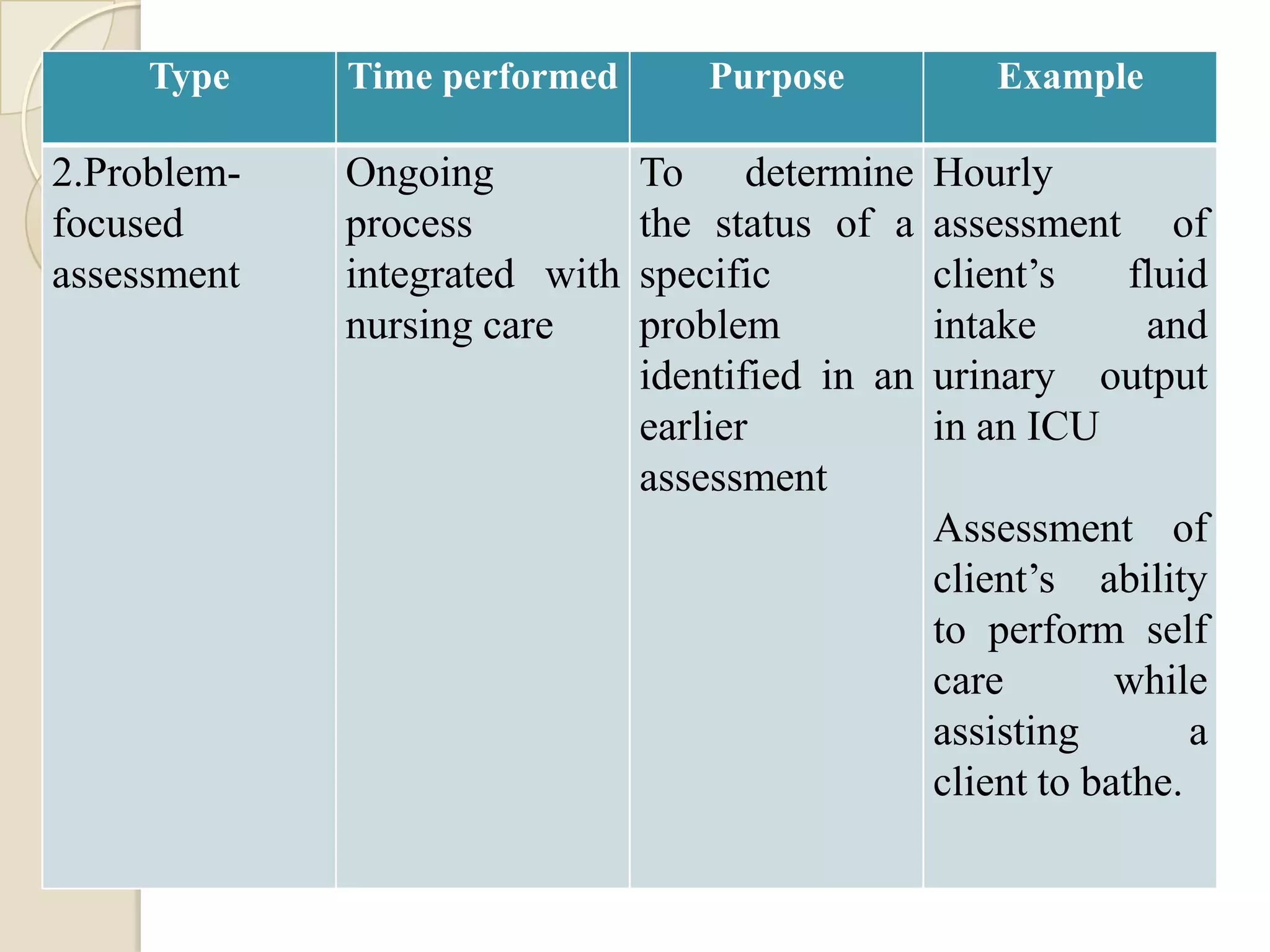
2] Problem focused assessment
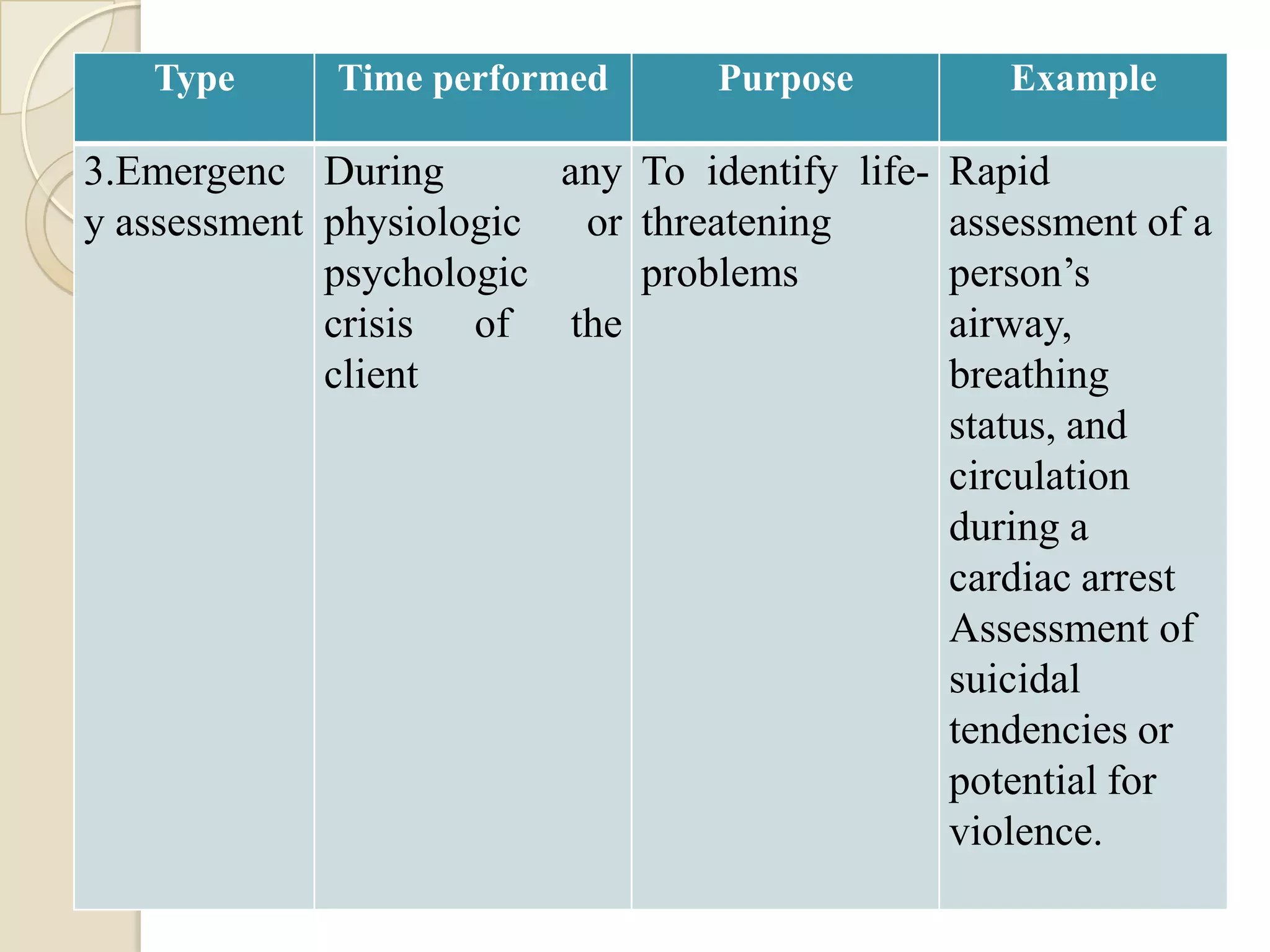
3] Emergency assessment
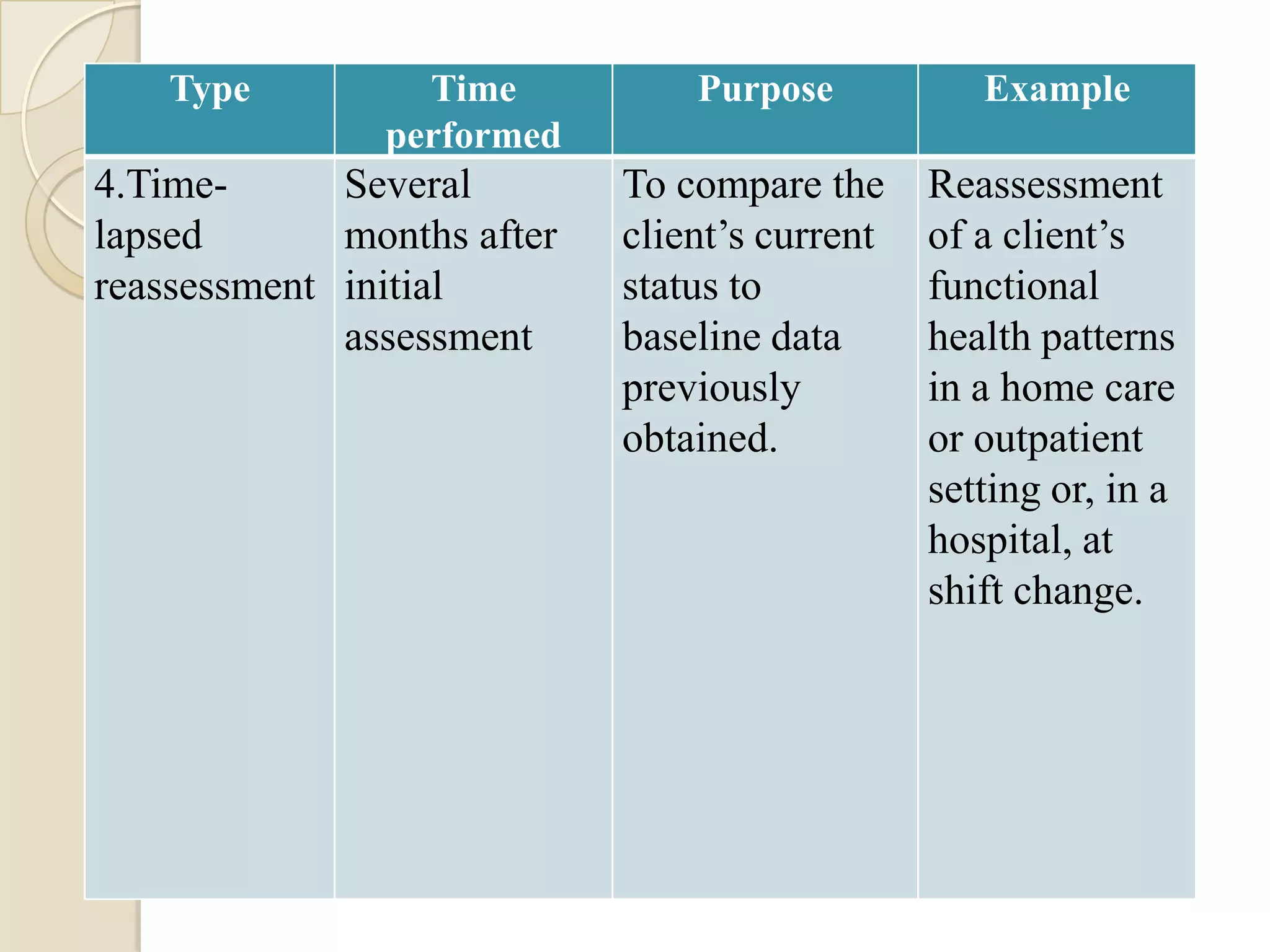
4] Time lapsed reassessment](https://image.slidesharecdn.com/nursingprocess-assessing-111105015609-phpapp01/75/Nursing-process-assessing-25-2048.jpg)
![i. c.Aspects of Observation
1] Noticing the data
2] Selecting, organizing & interpreting the
data
Eg : - A nurse who observes that a client’s
face is flushed, must relate that observation
to body temperature, activity, environmental
temperature, and blood pressure.
Errors can occur in selecting, organizing &
interpreting data.](https://image.slidesharecdn.com/nursingprocess-assessing-111105015609-phpapp01/75/Nursing-process-assessing-47-2048.jpg)
![ Nursing observations must be organized so that nothing
significant is missed.
Most nurses develop a particular sequence for observing
events, usually focusing on the client first.
For Eg. A nurse walks into a client’s room and observes, in
the following order.
1]Clinical signs of client distress (Eg. pallor or flushing, labored
breathing, and behavior indicating pain or emotional distress)
2] Threats to clients safety, real or anticipated (Eg. a lowered side rail)
3]The presence and functioning of associated equipment (Eg.
Equipment & oxygen)
4] The immediate environment, including the people in it.](https://image.slidesharecdn.com/nursingprocess-assessing-111105015609-phpapp01/75/Nursing-process-assessing-48-2048.jpg)
![Stages of an interview
Opening or introduction 2 steps
1] establish rapport
2] orientation
Body or development – closing](https://image.slidesharecdn.com/nursingprocess-assessing-111105015609-phpapp01/75/Nursing-process-assessing-55-2048.jpg)