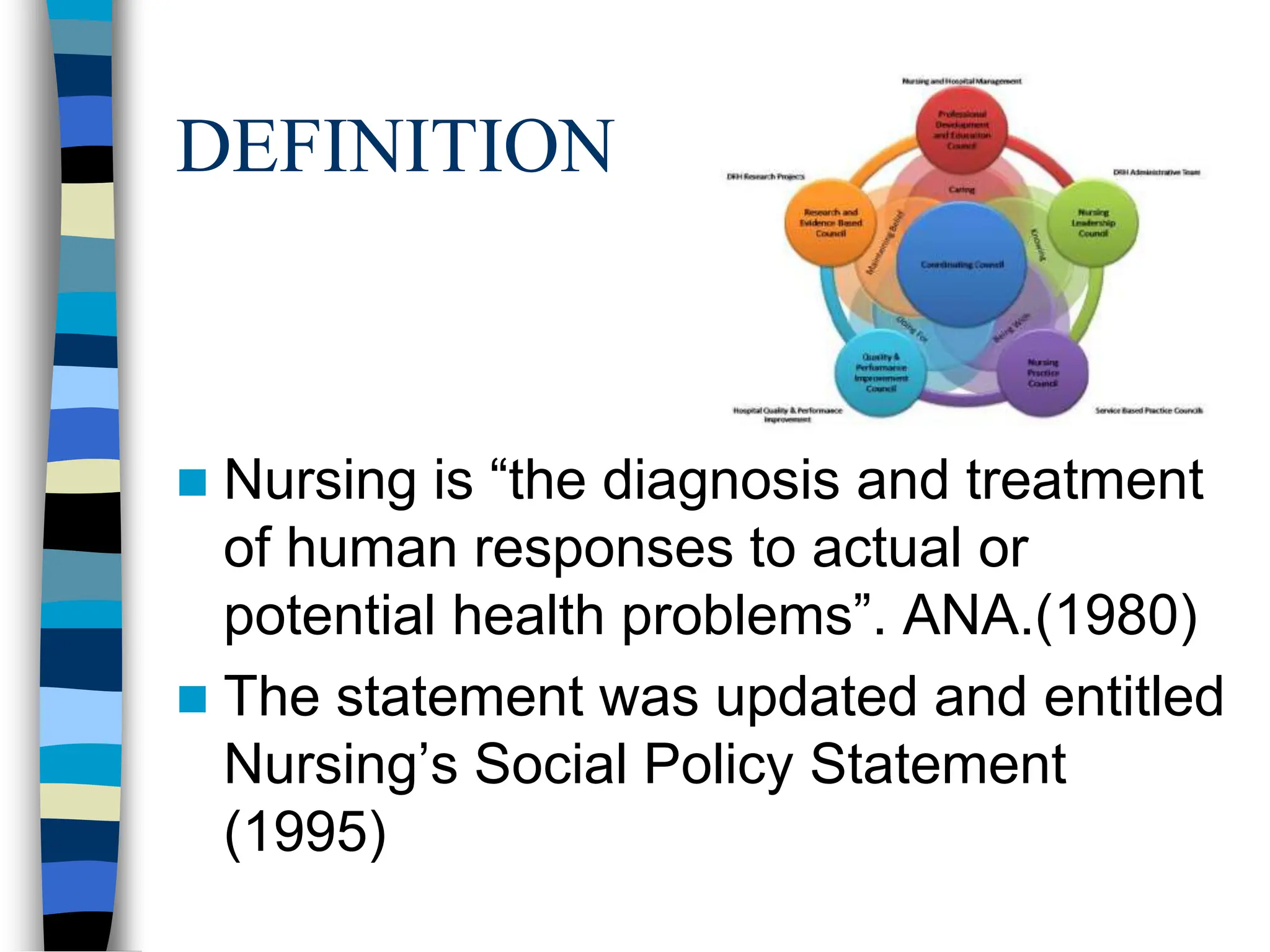
The document discusses the definition of nursing, the nursing process, and its key components. It defines nursing as the diagnosis and treatment of human responses to health problems. The nursing process is described as a systematic problem-solving approach consisting of assessment, nursing diagnosis, planning, implementation, and evaluation. Each step of the nursing process is explained in detail, including how to write nursing diagnoses and establish goals, interventions, and expected outcomes.