Downloaded 919 times
![Measures of association
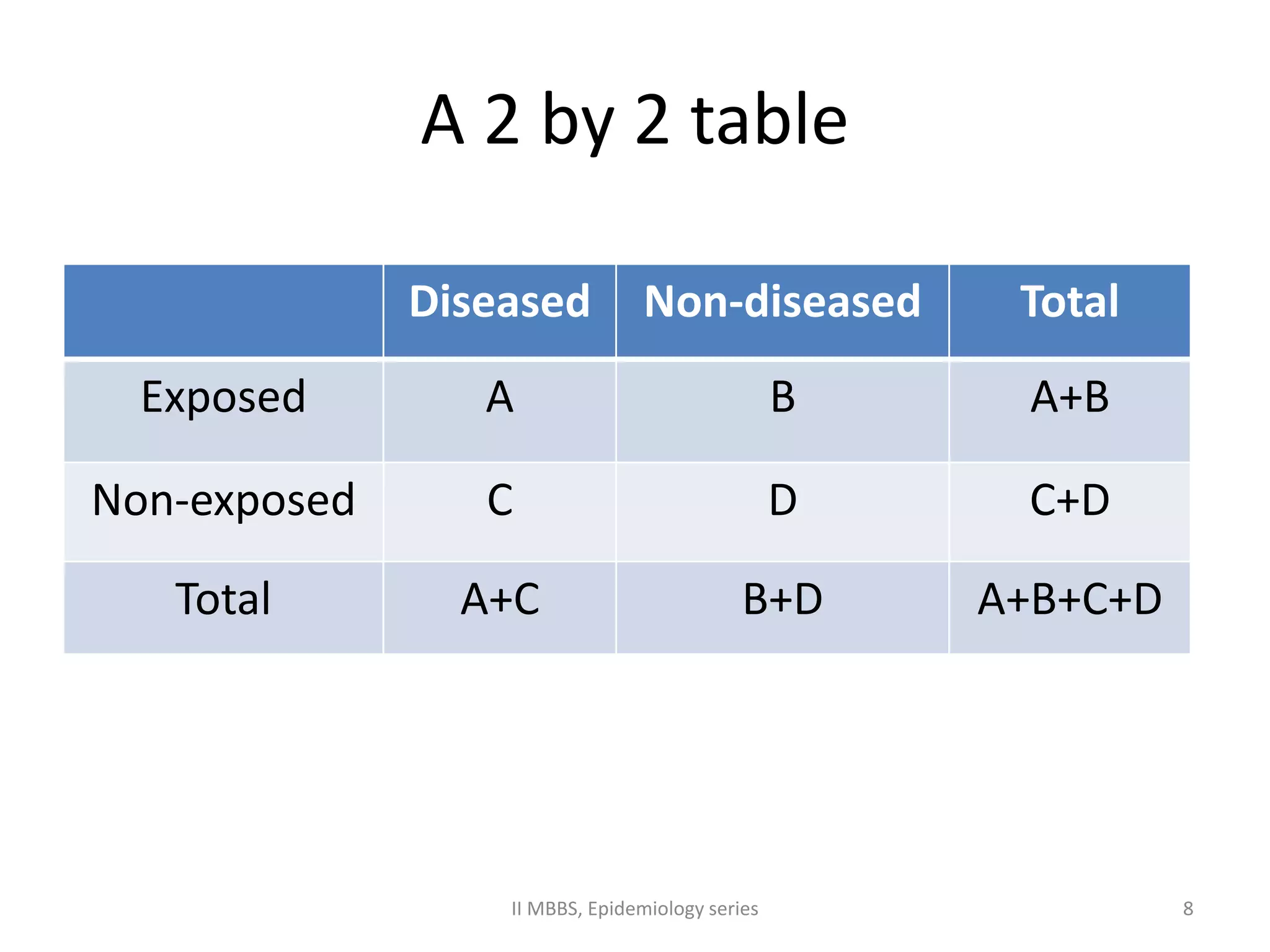
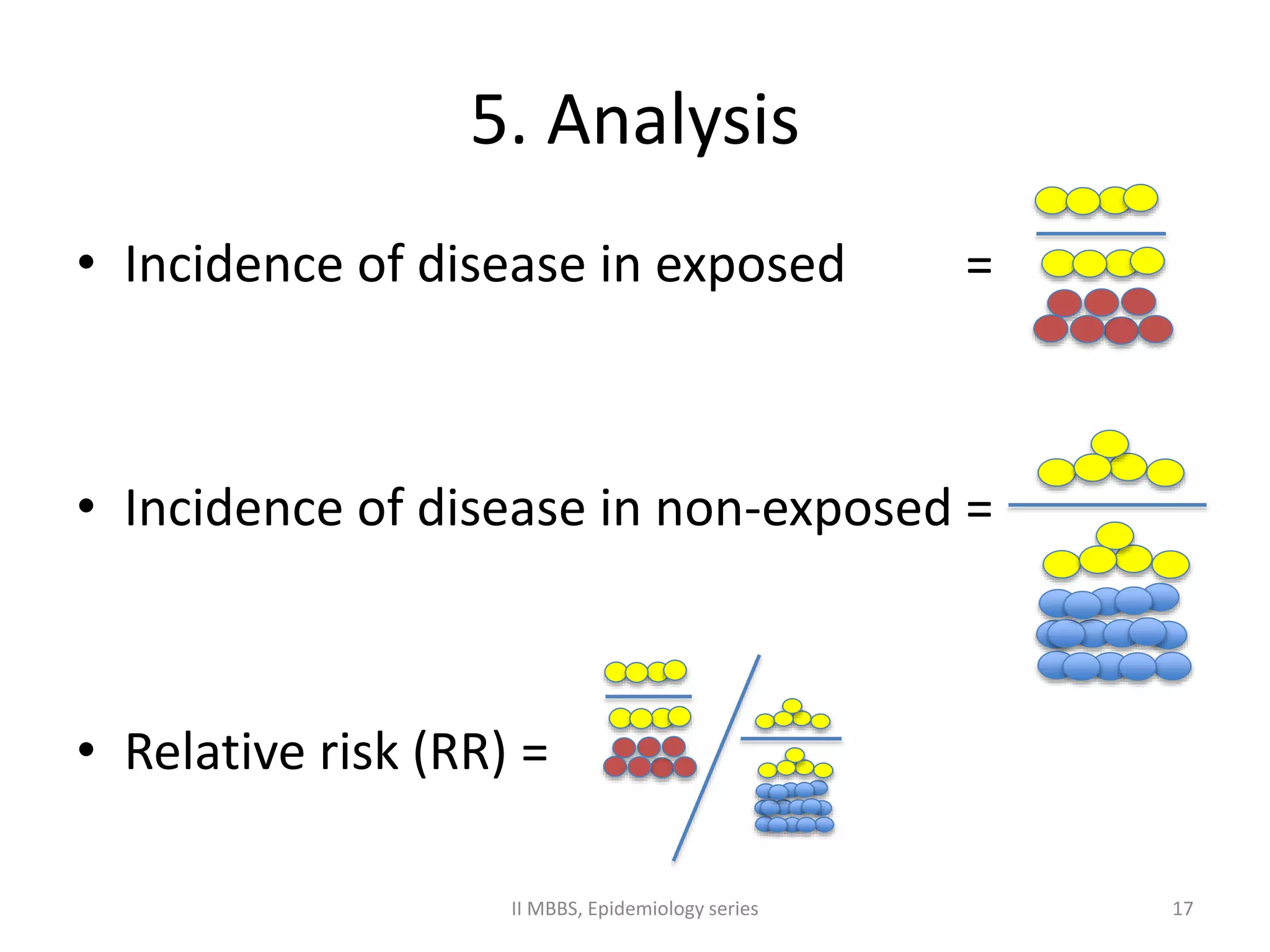
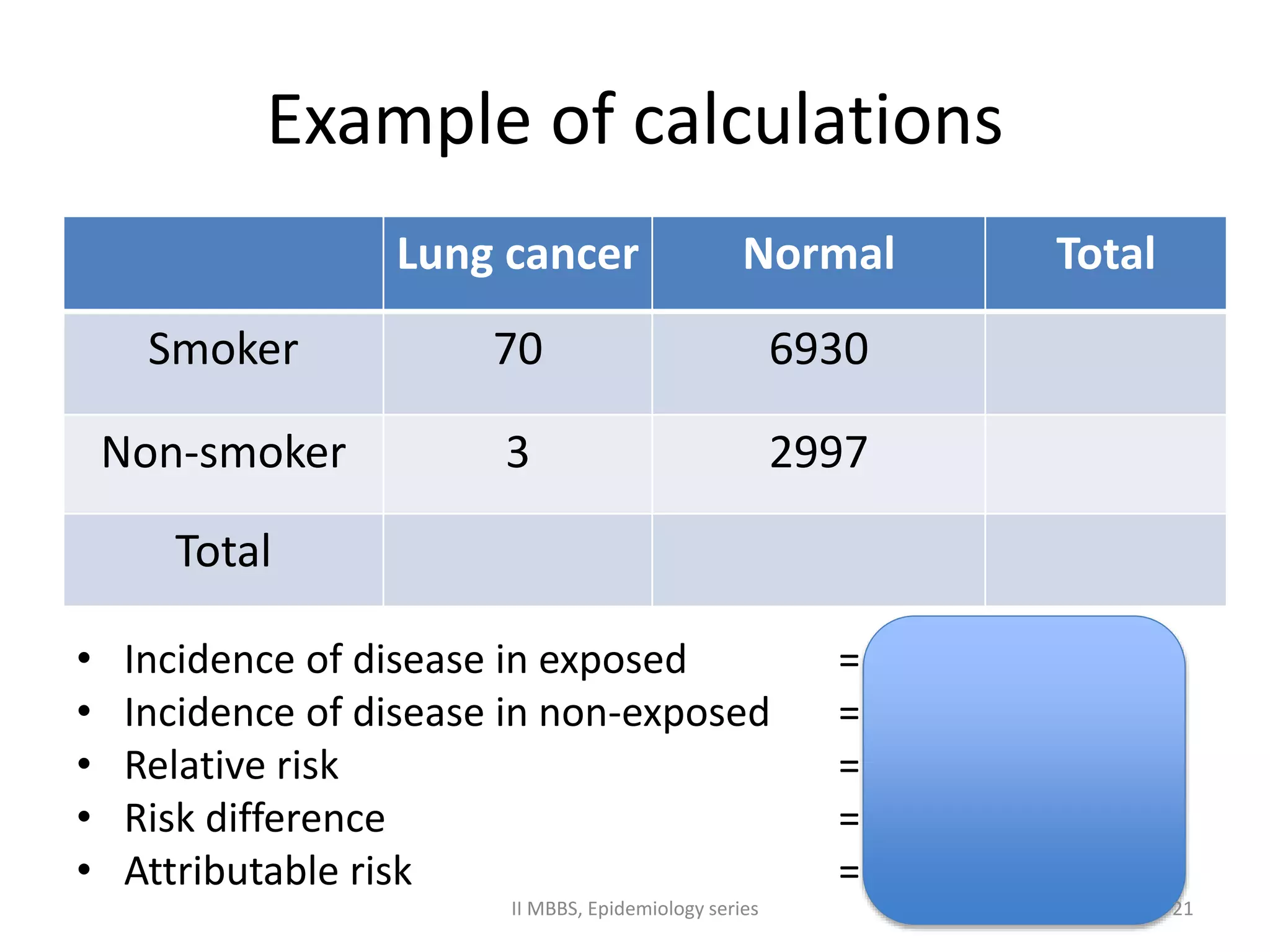
• Relative risk (RR) = I (e) / I (ue)
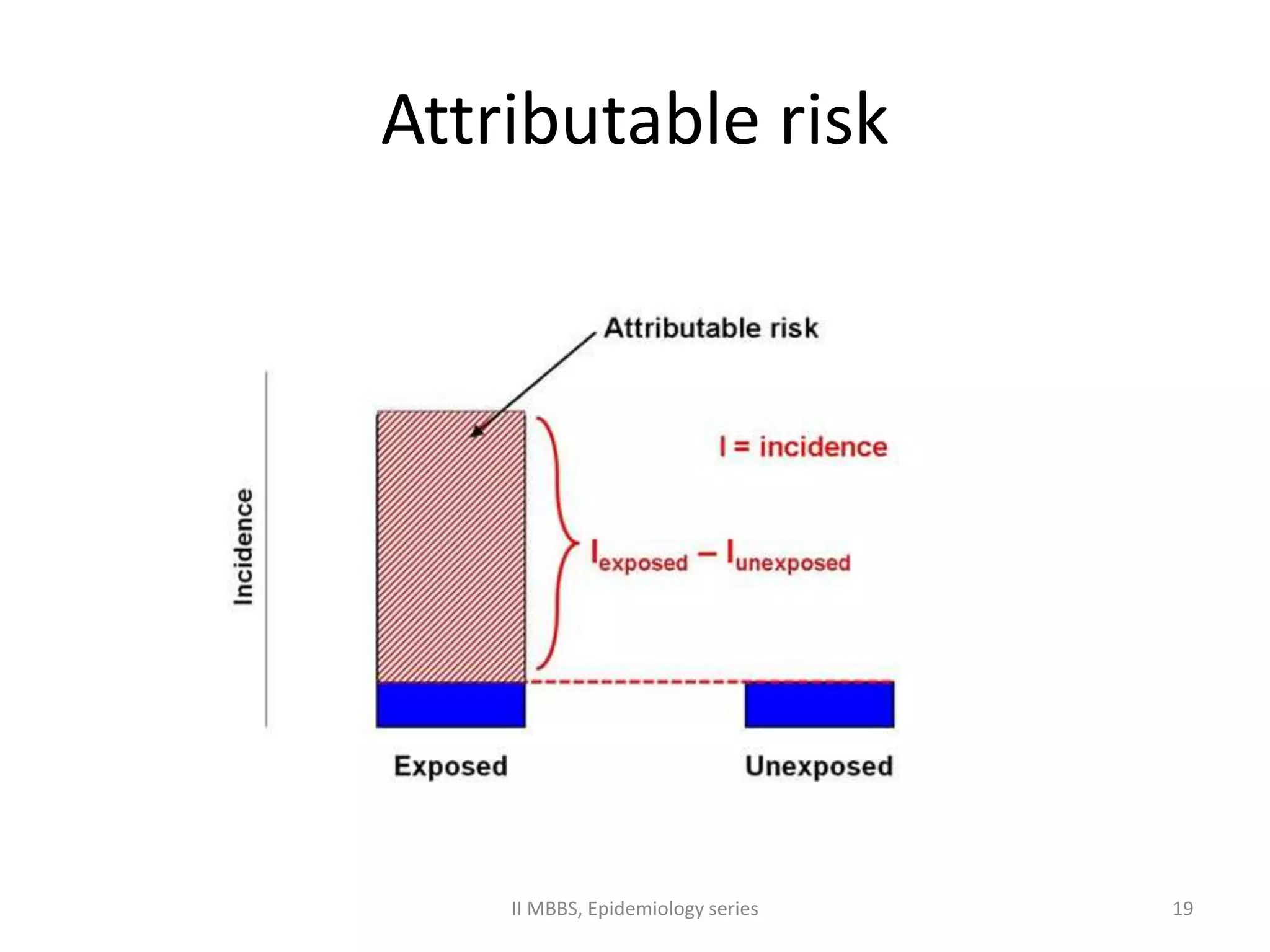
• Risk difference = I (e) - I (ue)
• Attributable risk = [I (e) – I (ue)]/ I (e)
• Population attributable risk
= Pe (RR-1) / Pe (RR-1) + 1
II MBBS, Epidemiology series 18](https://image.slidesharecdn.com/2ndyrcohort-141111214136-conversion-gate01/75/Cohort-study-basics-18-2048.jpg)

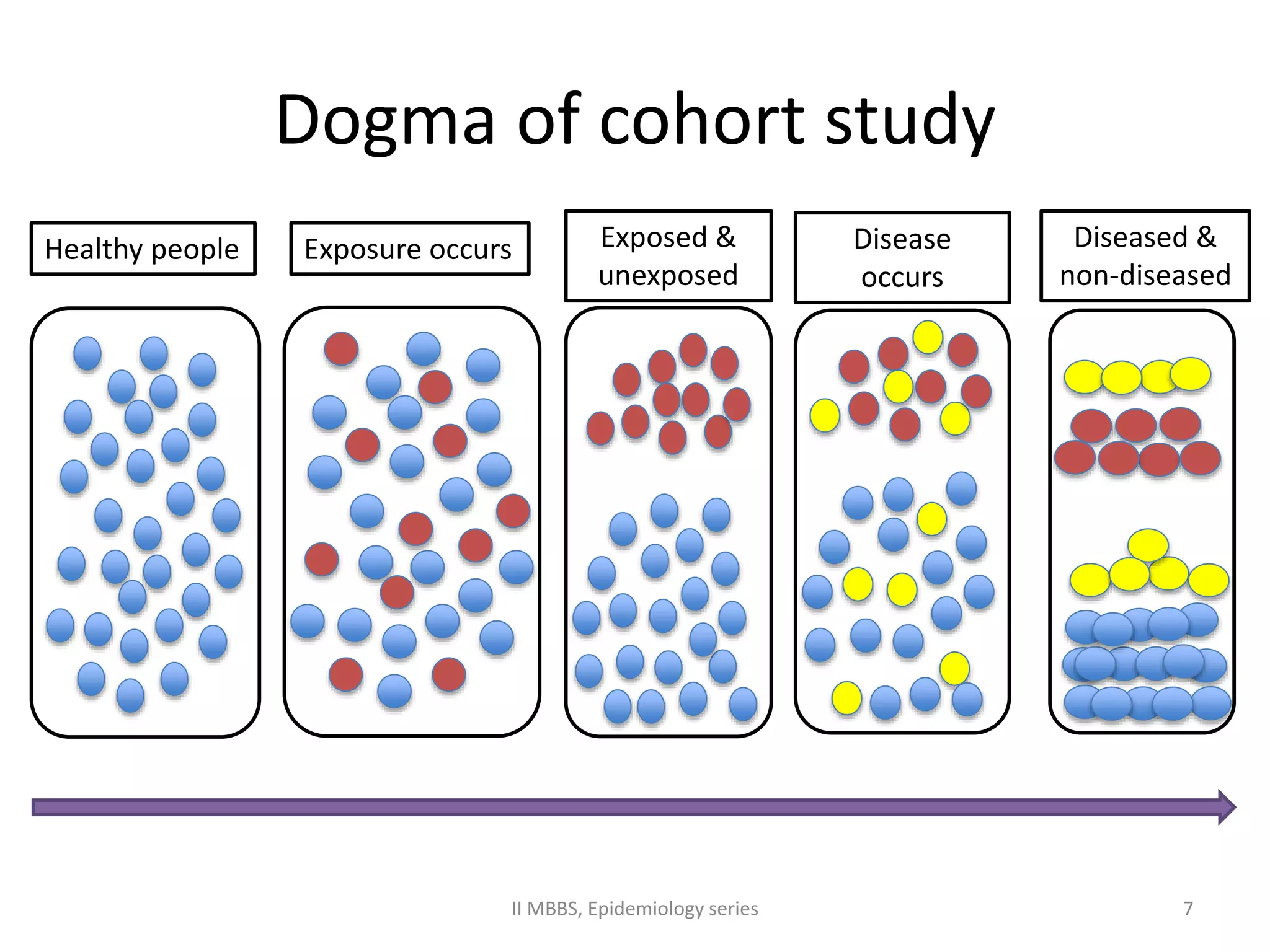
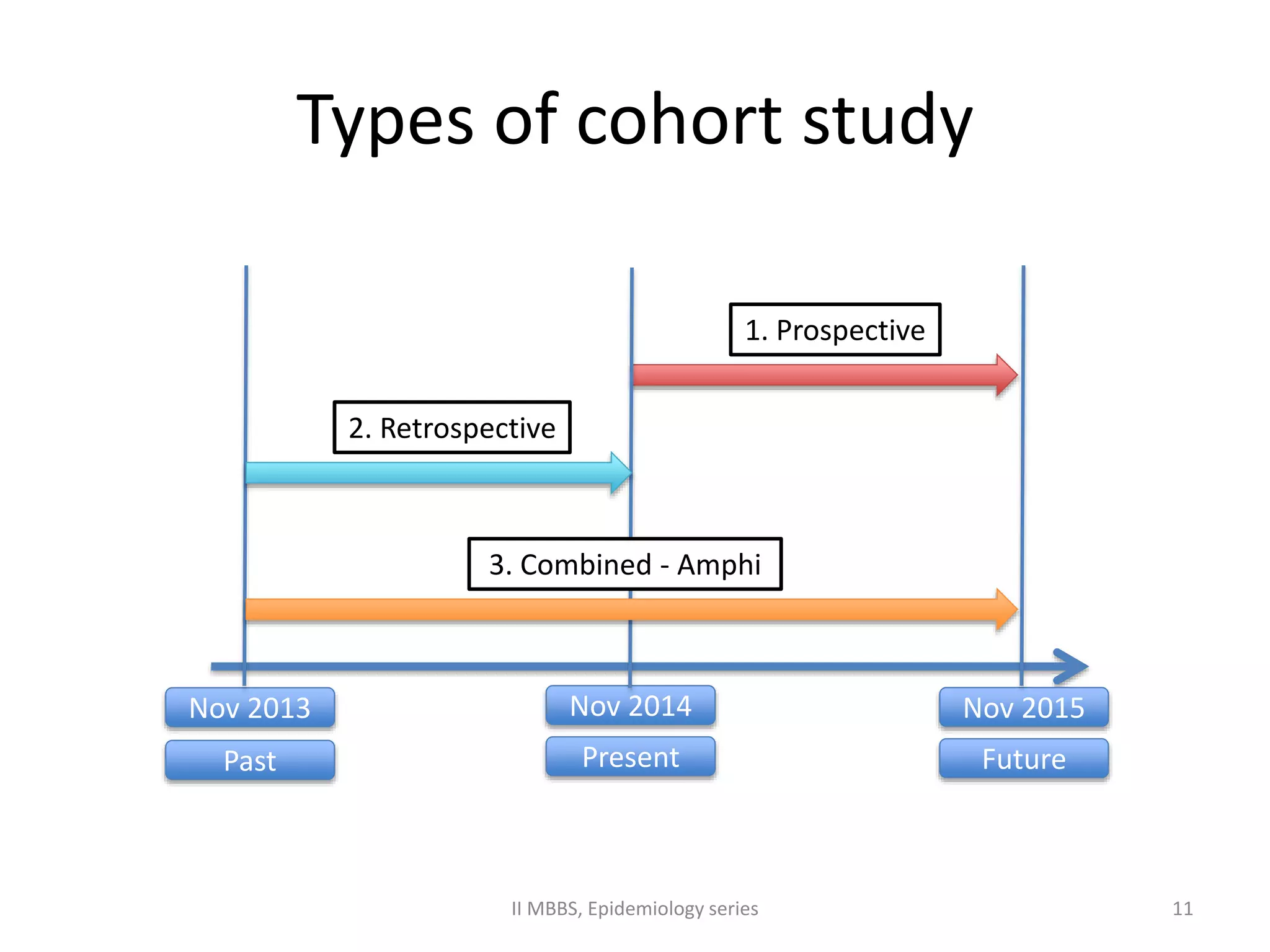
This document contains 26 slides presented by Dr. Rizwan S A on cohort studies. It defines cohort studies as prospective longitudinal studies that follow healthy populations over time to determine the causes of diseases. Key aspects covered include classifying cohort studies as prospective, retrospective or combined; describing the elements of cohort studies such as selecting and following subjects, measuring exposure and outcomes, and analyzing results using measures like relative risk, risk difference and attributable risk. Examples of famous cohort studies on smoking, heart disease and oral contraceptives are also provided.























































































