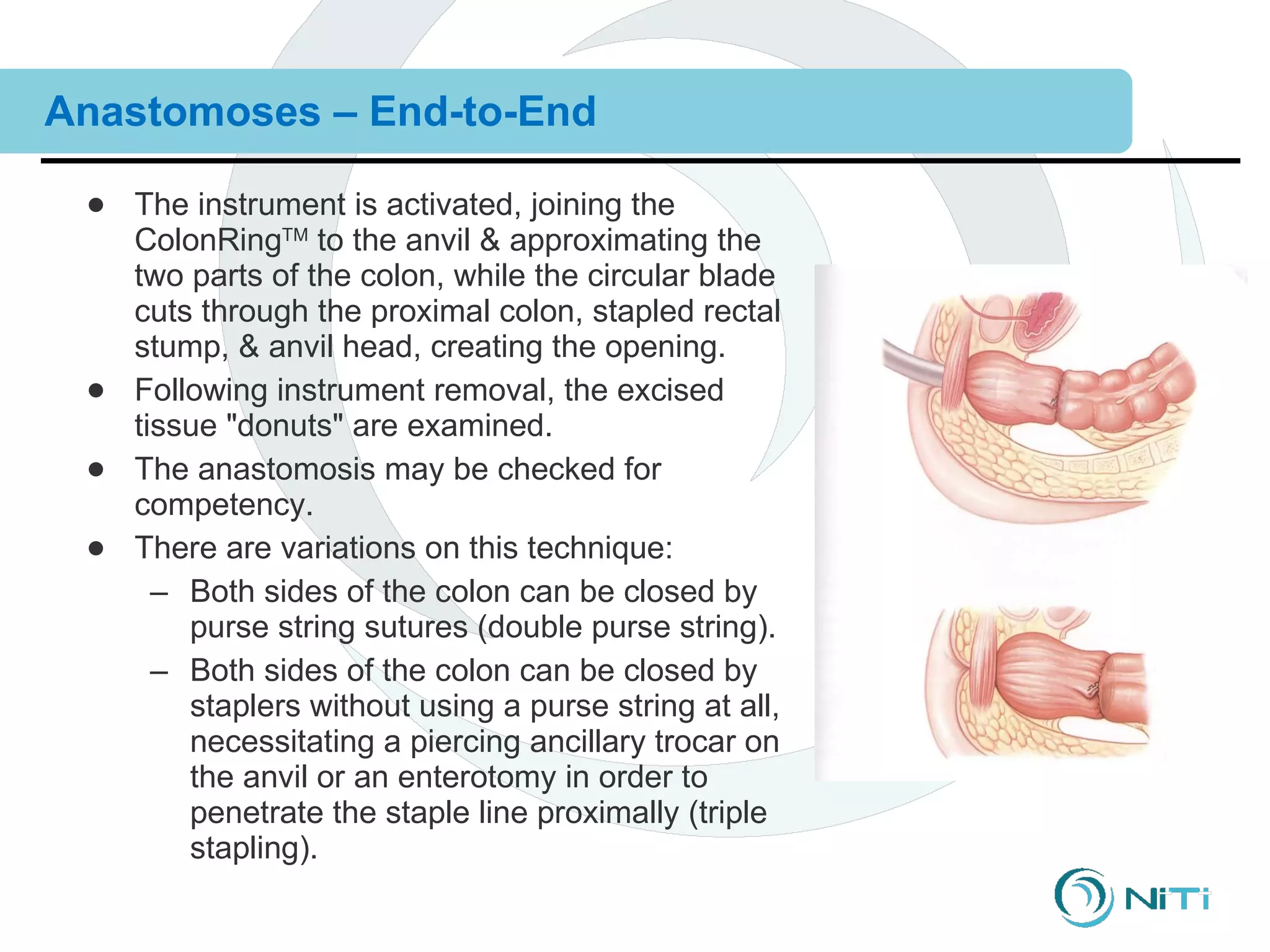
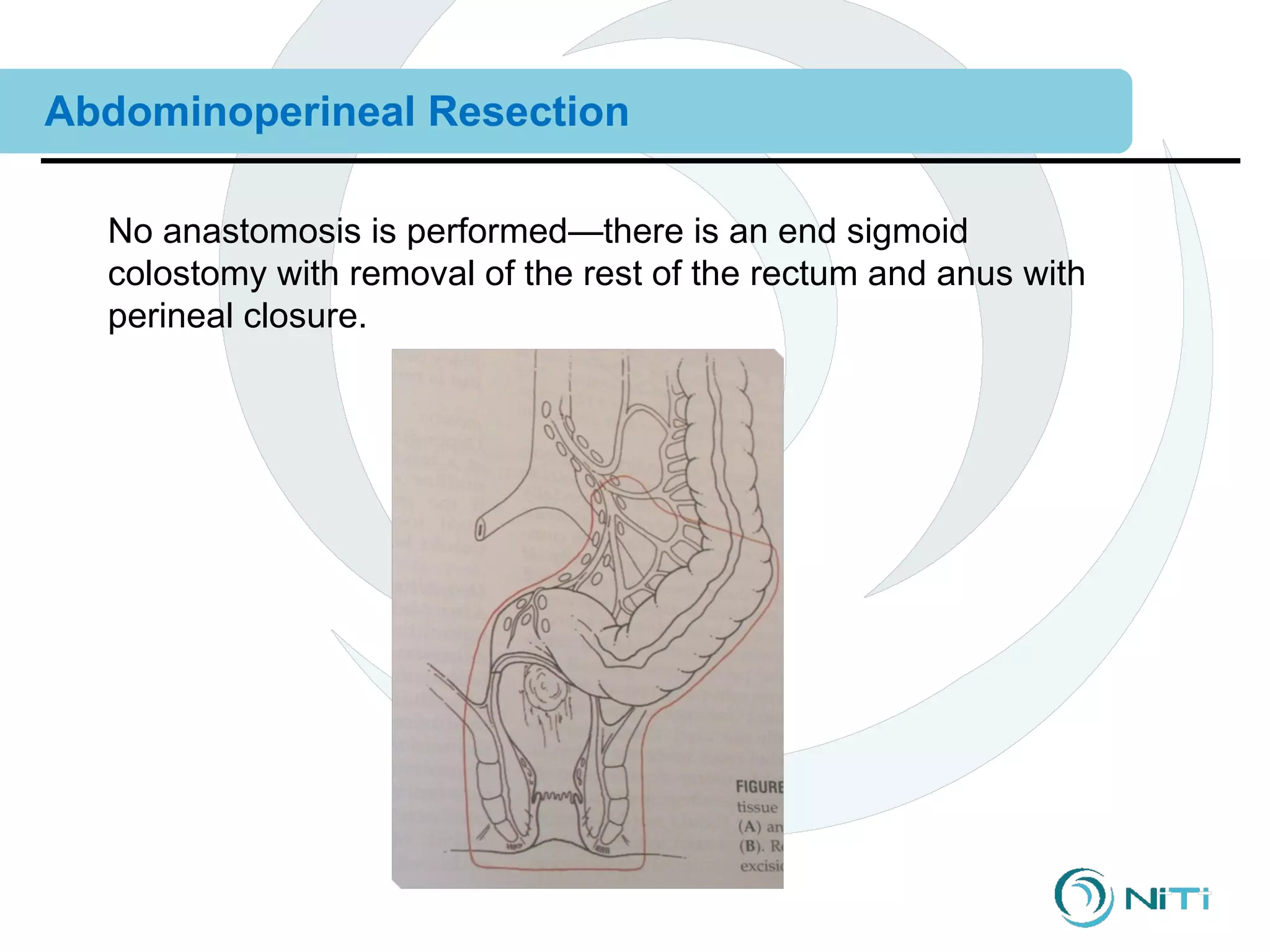
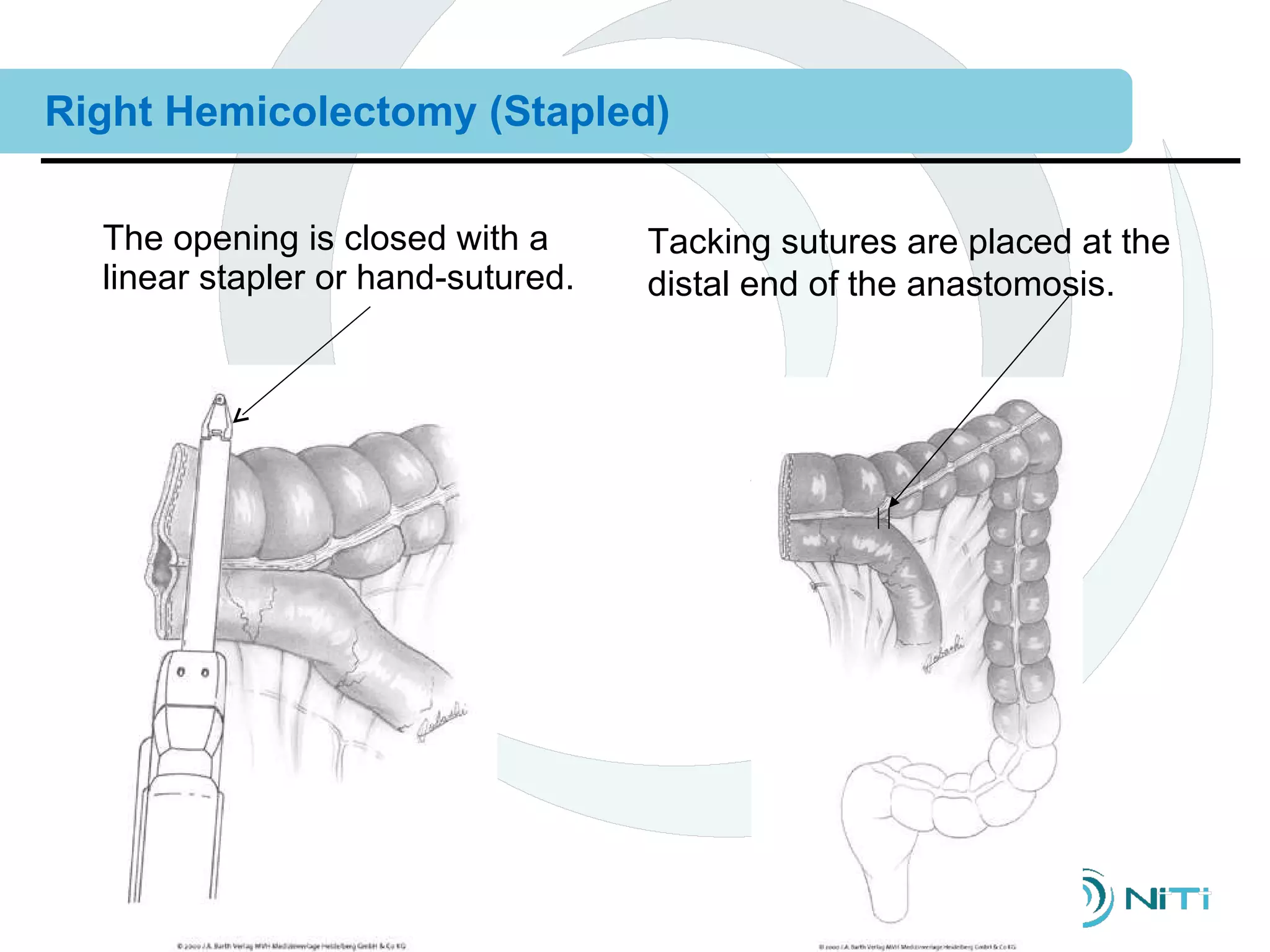
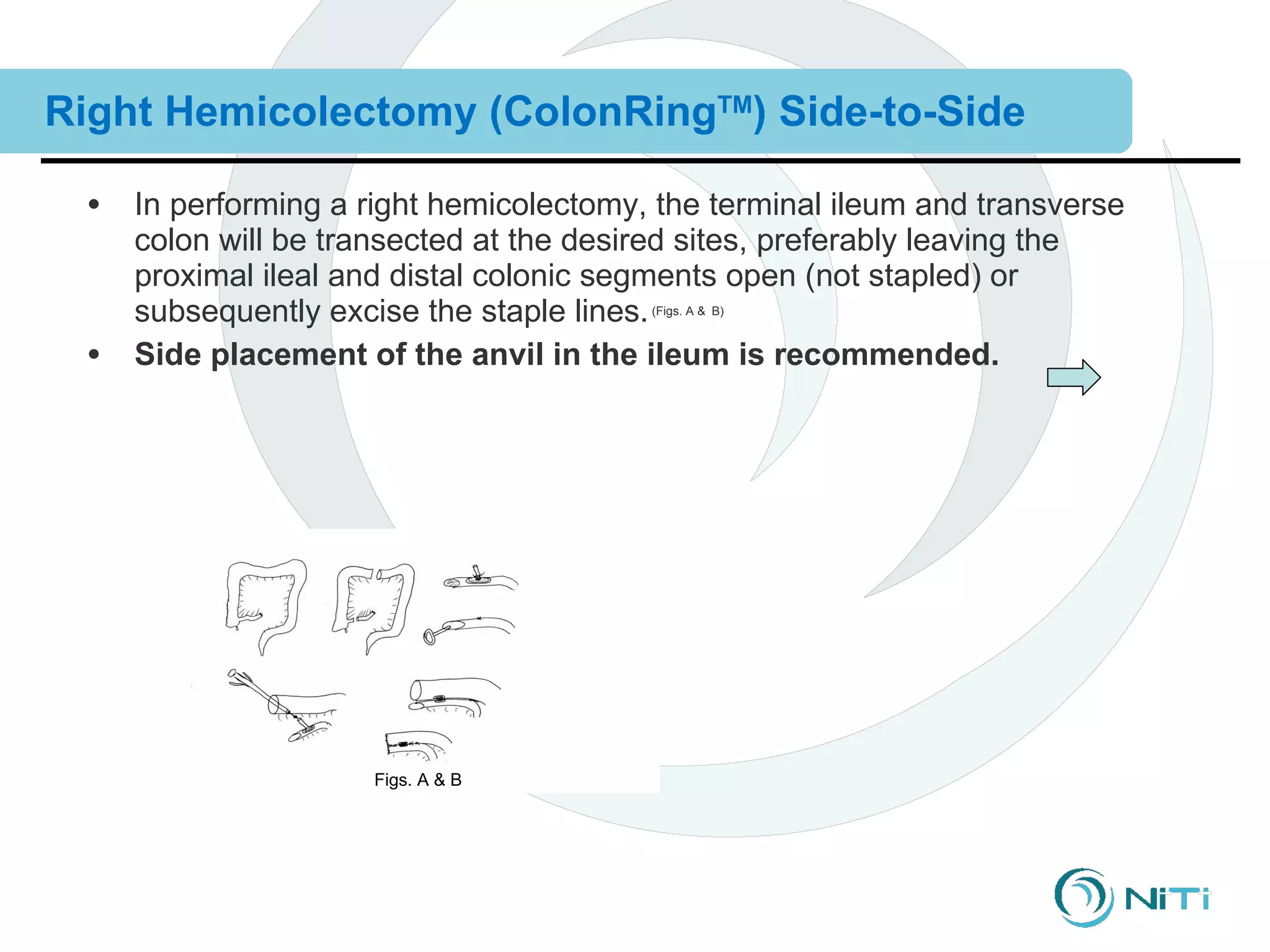
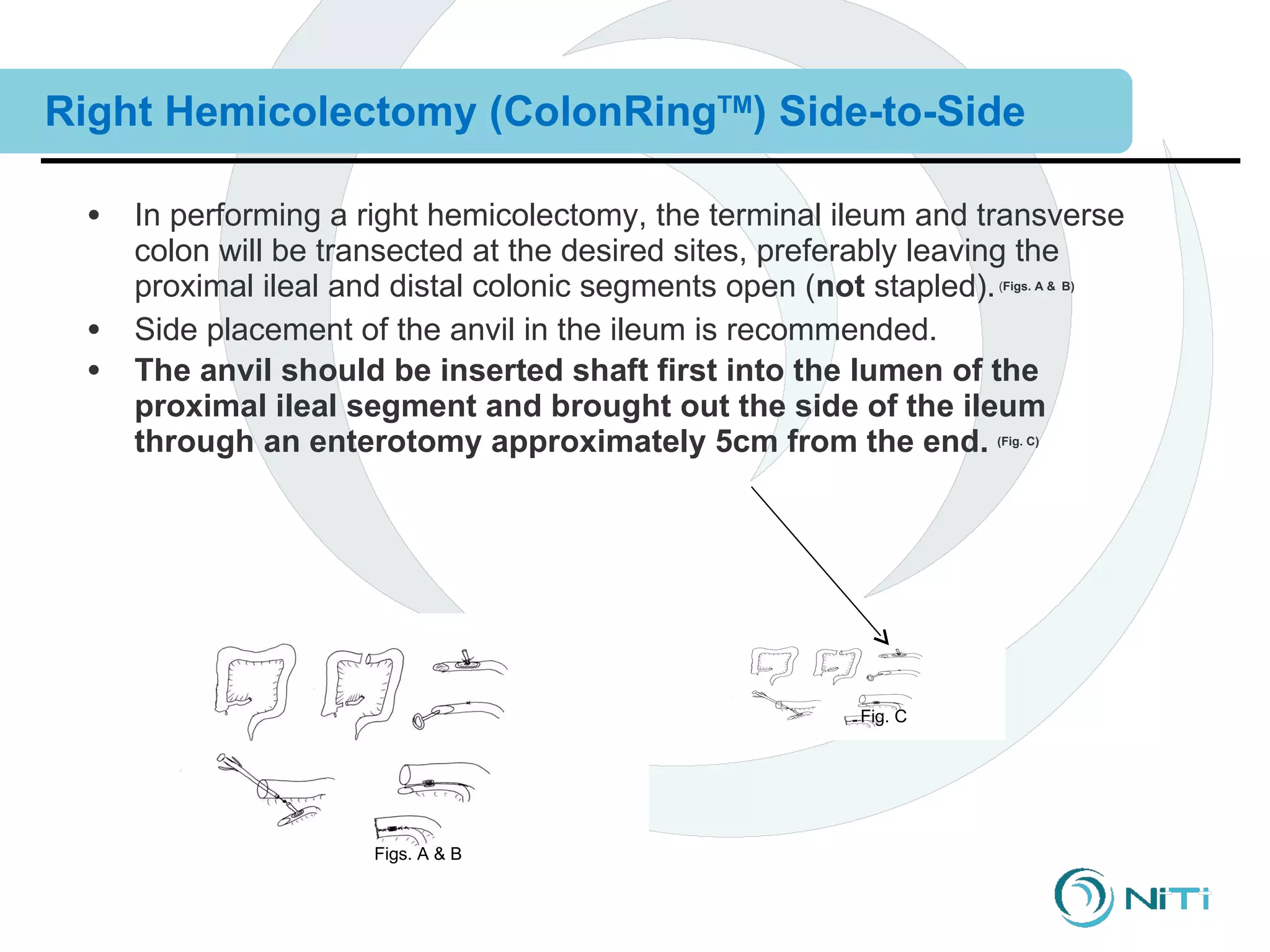
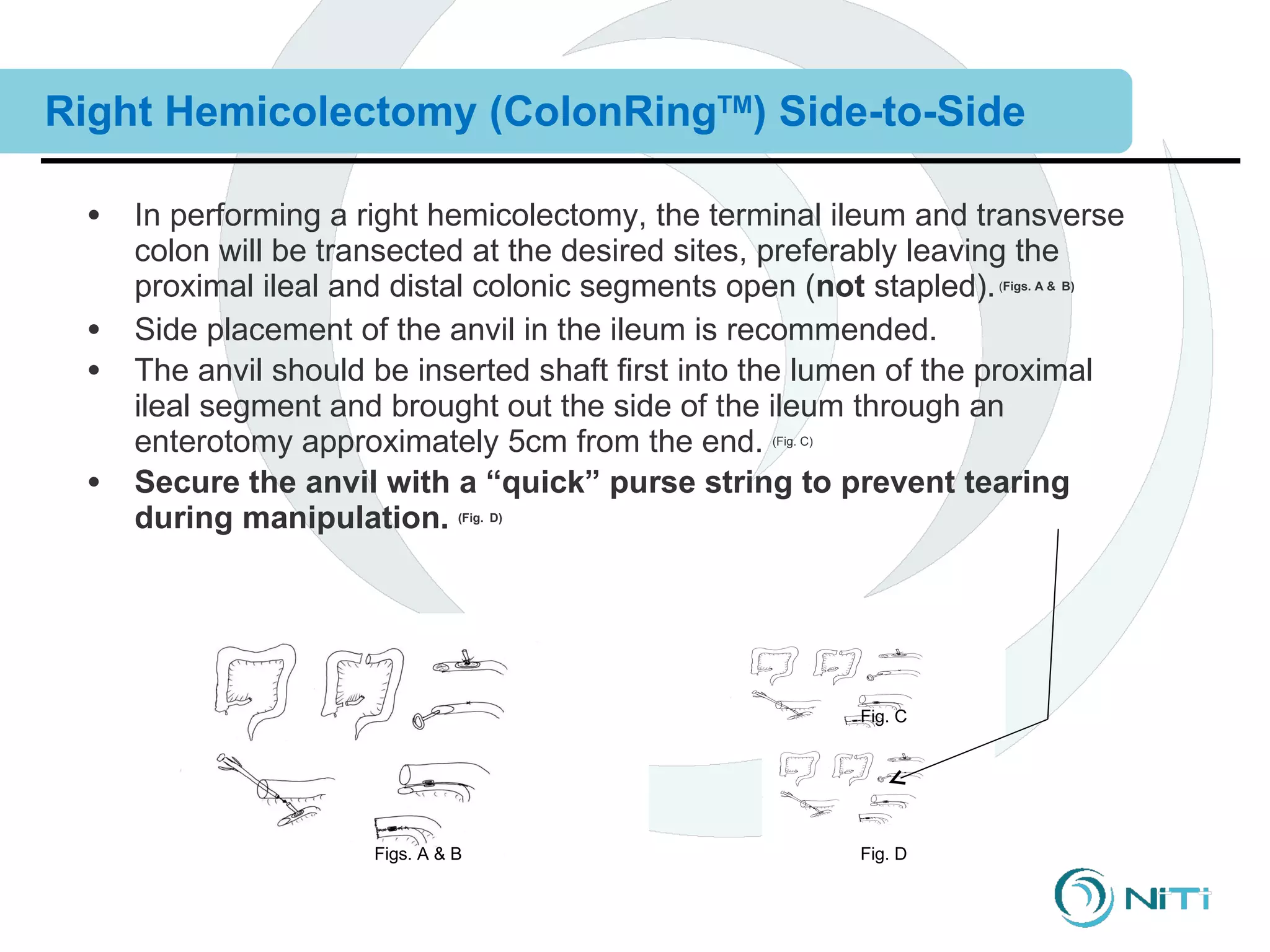
The document discusses various gastrointestinal surgical procedures that can be performed using the ColonRing device for intestinal anastomoses. It describes the basic steps for end-to-end, end-to-side, and side-to-side anastomoses. It then lists procedures that are and are not appropriate for the ColonRing device and provides more details on techniques for low anterior resection, total colectomy with ileoproctostomy, and procedures requiring special considerations.


































































































![Basics of Stoma and Management care[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/basicsofstomaandmanagement1-250417022629-8799f789-thumbnail.jpg?width=640&height=640&fit=bounds)













































