QUESTIONS ASKED
PREVIOUSLY(20 MARKS)
•Discuss in detail various pulp pathologies
and management in primary dentition
• Pain experienced due to pulpalgia in a
child
• Pathways of pulp in deciduous teeth and
how it affects endodontic treatment
• Discuss the scope and limitations of
pediatric endodontics
3.
QUESTIONS ASKED
PREVIOUSLY
• 100markers
• Dental Pulp in health and disease
• Diagnostic aids used in pediatric dentistry
• Recent concepts and controversies in pediatric endodontics
• Recent advances in pediatric endodontics
• 7 markers
• Recent concepts in pulp vitality testing
• Limitations of pulp vitality tests in children
• Internal root resorbtion
• Calcium hydroxide based internal resorbtion
4.
CONTENTS
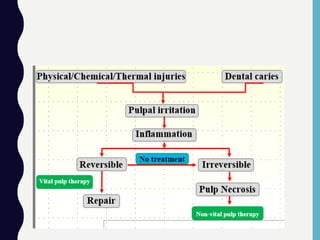
• Introduction topulpal diseases
• Reversible pulpitis
• Irreversible pulpitis
• Pulpal necrosis
• Diagnosis
• Diagnostic method
• Medical history
• Drugs & medication history
• Dental history
• Subjective symptoms
• Clinical observations
• Clinical tests
5.
DENTAL PULP
• ThePulp is a soft mesenchymal connective tissue that occupies
pulp cavity in the central part of the teeth.
6.
‘‘The pulp livesfor the dentin and the
dentin lives by the
grace of the pulp. Few marriages in nature
are marked
by a greater affinity.’’ Alfred L. Ogilvie
Average intrapulpal
pressure =10mm Hg
13 mm in reversible
35+ mm Hg
irreversible
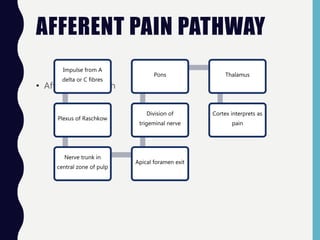
AFFERENT PAIN PATHWAY
•Afferent pain path
Impulse from A
delta or C fibres
Plexus of Raschkow
Nerve trunk in
central zone of pulp
Apical foramen exit
Division of
trigeminal nerve
Pons Thalamus
Cortex interprets as
pain
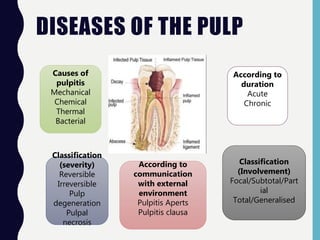
DISEASES OF THEPULP
Causes of
pulpitis
Mechanical
Chemical
Thermal
Bacterial
Classification
(severity)
Reversible
Irreversible
Pulp
degeneration
Pulpal
necrosis
Classification
(Involvement)
Focal/Subtotal/Part
ial
Total/Generalised
According to
duration
Acute
Chronic
According to
communication
with external
environment
Pulpitis Aperts
Pulpitis clausa
11.
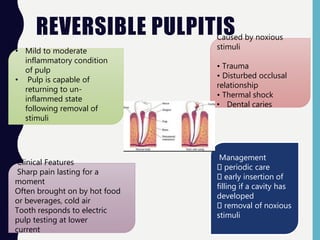
REVERSIBLE PULPITIS
• Mildto moderate
inflammatory condition
of pulp
• Pulp is capable of
returning to un-
inflammed state
following removal of
stimuli
Caused by noxious
stimuli
• Trauma
• Disturbed occlusal
relationship
• Thermal shock
• Dental caries
Clinical Features
Sharp pain lasting for a
moment
Often brought on by hot food
or beverages, cold air
Tooth responds to electric
pulp testing at lower
current
Management
periodic care
early insertion of
filling if a cavity has
developed
removal of noxious
stimuli
12.
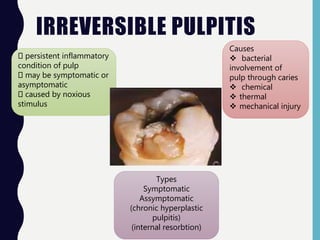
IRREVERSIBLE PULPITIS
persistent inflammatory
conditionof pulp
may be symptomatic or
asymptomatic
caused by noxious
stimulus
Causes
bacterial
involvement of
pulp through caries
chemical
thermal
mechanical injury
Types
Symptomatic
Assymptomatic
(chronic hyperplastic
pulpitis)
(internal resorbtion)
13.
IRREVERSIBLE PULPITIS
Early Stagepain
• sharp
• piercing
• shooting
• generally severe
• bending over or lying down exacerbates
pain which is
due to change in
intrapulpal pressure
Late stage pain
More severe or throbbing as if tooth is under
constant pressure
Patient is often awake at night due to pain
Increased by heat & sometimes relieved by
cold
Continued cold applied may exacerbate pain
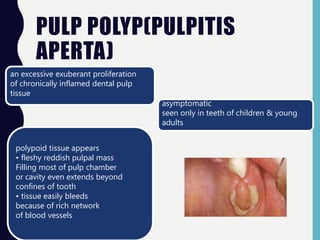
PULP POLYP(PULPITIS
APERTA)
an excessiveexuberant proliferation
of chronically inflamed dental pulp
tissue
asymptomatic
seen only in teeth of children & young
adults
polypoid tissue appears
• fleshy reddish pulpal mass
Filling most of pulp chamber
or cavity even extends beyond
confines of tooth
• tissue easily bleeds
because of rich network
of blood vessels
16.
INTERNAL RESORPTION
• Idiopathicslow or fast progressive resorptive process occuring
in
dentin of the pulp chamber or pulp canal of the tooth.
• Exhibit no additional symptoms other than existing pulpitis.
• Crown may appear as pink ,when resorption is in coronal
portion.(Pink tooth)
• Resorption involving the root canal appears as round to oval R/L
area that extends from pulp canal.
17.
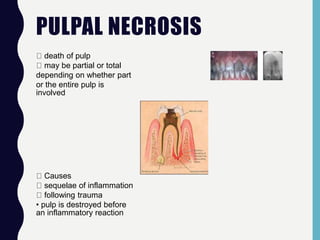
PULPAL NECROSIS
death ofpulp
may be partial or total
depending on whether part
or the entire pulp is
involved
Causes
sequelae of inflammation
following trauma
• pulp is destroyed before
an inflammatory reaction
18.
TYPES OF NECROSIS
CoagulationNecrosis
•soluble portion of
tissue is precipitated
or converted into a solid
material
• tissue is converted into tissue
mass consisting chiefly of
coagulated
•proteins
•fats
•water
LiquefactionNecrosis
•results when proteolytic
enzymes convert the tissue into
softened mass
•liquid or amorphous debris
20.
Diagnosis:
‘The art andscience of
detecting
deviations from health
and the cause and
nature thereof’
HISTORY OF PRESENT
ILLNESS• Duration
• Mode of onset
• Progression
• Severity
• Nature
• Aggravating/relieving factors
• Postural variation
• Any medications/treatment received for the same
Elaboration of
complaint(pain)
25.
PAIN
• Most commoncomplaint that leads to dental
treatment
• According to intensity
Mild pain
• Controlled
by simple
analgesics
Moderate
pain
• Controlled
with narcotic
analgesics
Severe pain
• Cannot
controlled
with
analgesics
• Require
elimination
of cause
26.
According to nature
•Pricking/piercing
• Throbbing
• Lancinating
• Aching
• Dull, boring, gnawing
Localization of pain
• Localised when patient can
point to a specific tooth or site
• Sharp , piercing and
lancinating pain in a tooth
responds to cold and is easy to
localize
• Dull, boring pain is diffuse and
responds abnormally to heat
than to cold is difficult to
localize.
27.
ACCORDING TO DURATION
•Pain of short duration & separated by
wholly pain free period
Intermittent
• Pain of longer durationContinuous
• Two or more similar episodes of painRecurrent
Periodic • Characterized by regularly
recurring episode
28.
ACCORDING TO ONSET
•Pain occurs
without being
provoked
Spontaneous
• Provocation causes
painful sensation
Induced
• When evoked
response is out of
proportion to the
stimulus
Triggered
29.
SWELLING
Anatomical location(site)
Duration
Mode of onset
Symptoms
Progress of swelling
Associated features
Secondary changes
Impairment of function
Recurrence of swelling
30.
PAST MEDICAL HISTORY
-Anemia
-Bleedingdisorders
-Cardio respiratory disorders
-Drug treatment and allergies
-Endocrine disorders
-Fits and faints
-Gastrointestinal disorders
-Hospital admissions and surgeries
-Infections
-Jaundice and liver diseases
-Kidney disease
Checklist by Scully & Cawson
31.
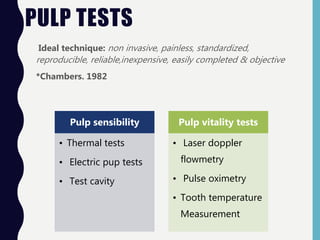
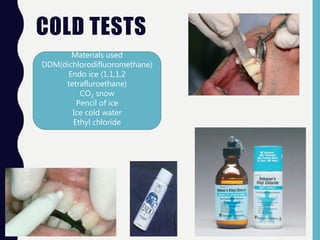
CLINICAL TESTS
Diagnostic tests:
1.EPT
2. Thermal tests
3. Percussion
4. Palpation
5. Mobility
6. Periodontal
evaluation
7. Occlusal evaluation
8. Radiograph
Selective tests for
Difficult Diagnostic
Situations:
9. Test cavity
preparation
10. Anesthetic test
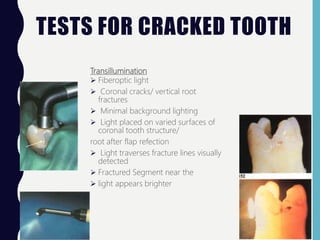
11. Transillumination
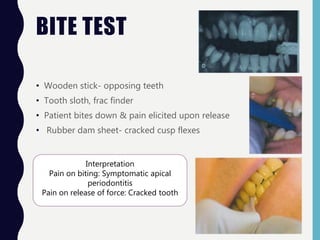
12. Biting
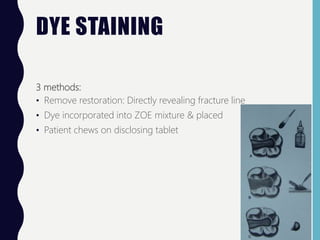
13.Staining
14. Gutta percha point
tracing with radiograph
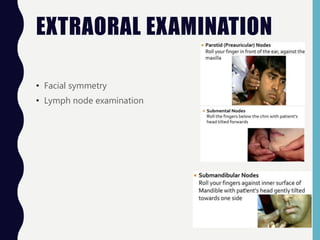
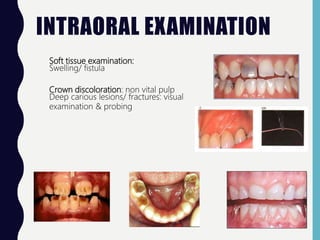
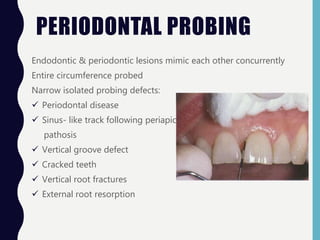
INTRAORAL EXAMINATION
Soft tissueexamination:
Swelling/ fistula
Crown discoloration: non vital pulp
Deep carious lesions/ fractures: visual
examination & probing
34.
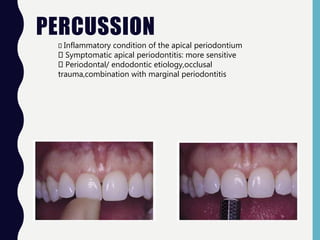
PERCUSSION
Inflammatory condition ofthe apical periodontium
Symptomatic apical periodontitis: more sensitive
Periodontal/ endodontic etiology,occlusal
trauma,combination with marginal periodontitis
35.
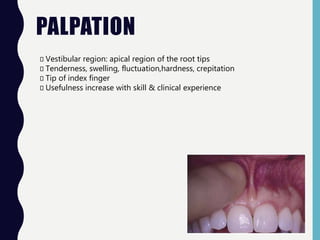
PALPATION
Vestibular region: apicalregion of the root tips
Tenderness, swelling, fluctuation,hardness, crepitation
Tip of index finger
Usefulness increase with skill & clinical experience
36.
MOBILITY
Miller’s index:
Class 1-First distinguishable sign of
greater- than- normal movement
Class 2- Movement of the crown as much
as 1mm in any direction
Class 3- Movement of the crown more
than 1 mm in any direction and/or vertical
depression/ rotation of the crown in its
socket
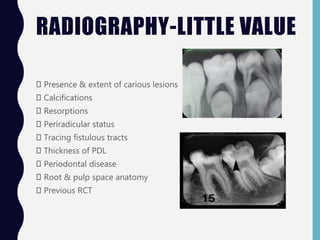
VALUE OF DIAGNOSTIC
TESTS
Specificity:The ability
of a test to detect
the absence of a result
Positive predictive value:
The probability
that a positive test result
actually
represents a disease
positive tooth
Negative predictive value:
The probability
that a tooth with a negative
test result is
actually free from the disease
Heat: relatively high
sensibility; but least
accurate being the least
specific
Cold test: more
accurate than EPT
43.
THERMAL TESTS RATIONALE
•C fibres (slower)
• Dull long lasting pain
Heat test
• A fibres faster
• Hydrodynamic movement of fluid in
dentinal tubules
• Sharp localized pain
Cold test
First reported by Jack in 1899
Often inappropriately referred to as ‘Vitality
tests’
More reliable than EPT
Inexpensive & easy-to- use equipment
Patient’s pain reproduced
44.
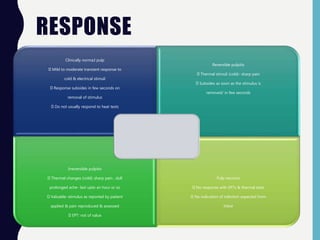
RESPONSE
Clinically norma;l pulp
Mildto moderate transient response to
cold & electrical stimuli
Response subsides in few seconds on
removal of stimulus
Do not usually respond to heat tests
Reversible pulpitis
Thermal stimuli (cold)- sharp pain
Subsides as soon as the stimulus is
removed/ in few seconds
Irreversible pulpitis
Thermal changes (cold): sharp pain , dull
prolonged ache- last upto an hour or so
Valuable: stimulus as reported by patient
applied & pain reproduced & assessed
EPT: not of value
Pulp necrosis
No response with EPTs & thermal tests
No indication of infection expected from
these
45.
RESPONSE
Pulp Necrobiosis
Difficult todiagnose
History : pulpitis
Pulp tests: necrosis
Vague response to
EPTs, cold tests
Acute apical periodontitis
Maybe associated with
pulpitis
Pulp status assessed
before treatment
Acute apical abscess-
Negative
Lateral periodontal abscess-
Positive
46.
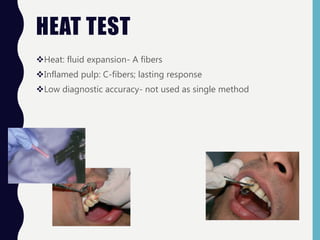
HEAT TEST
Heat: fluidexpansion- A fibers
Inflamed pulp: C-fibers; lasting response
Low diagnostic accuracy- not used as single method
47.
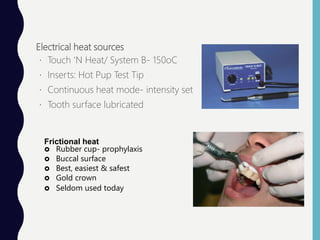
Electrical heat sources
Touch‘N Heat/ System B- 150oC
Inserts: Hot Pup Test Tip
Continuous heat mode- intensity set
Tooth surface lubricated
Frictional heat
Rubber cup- prophylaxis
Buccal surface
Best, easiest & safest
Gold crown
Seldom used today
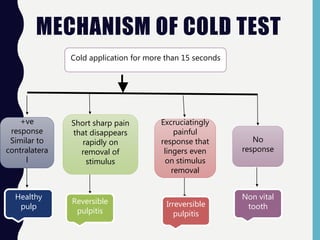
MECHANISM OF COLDTEST
Cold application for more than 15 seconds
+ve
response
Similar to
contralatera
l
Short sharp pain
that disappears
rapidly on
removal of
stimulus
Excruciatingly
painful
response that
lingers even
on stimulus
removal
No
response
Healthy
pulp
Reversible
pulpitis
Irreversible
pulpitis
Non vital
tooth
50.
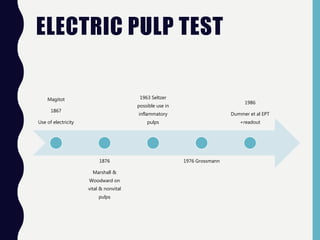
ELECTRIC PULP TEST
Magitot
1867
Useof electricity
1876
Marshall &
Woodward on
vital & nonvital
pulps
1963 Seltzer
possible use in
inflammatory
pulps
1976 Grossmann
1986
Dummer et al EPT
+readout
51.
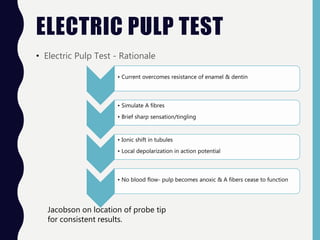
ELECTRIC PULP TEST
•Electric Pulp Test - Rationale
• Current overcomes resistance of enamel & dentin
• Simulate A fibres
• Brief sharp sensation/tingling
• Ionic shift in tubules
• Local depolarization in action potential
• No blood flow- pulp becomes anoxic & A fibers cease to function
Jacobson on location of probe tip
for consistent results.
52.
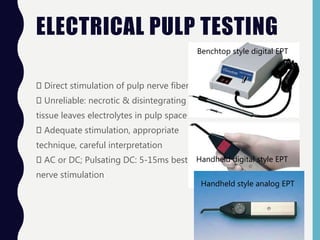
ELECTRICAL PULP TESTING
Directstimulation of pulp nerve fibers
Unreliable: necrotic & disintegrating pulp
tissue leaves electrolytes in pulp space
Adequate stimulation, appropriate
technique, careful interpretation
AC or DC; Pulsating DC: 5-15ms best
nerve stimulation
Benchtop style digital EPT
Handheld digital style EPT
Handheld style analog EPT
53.
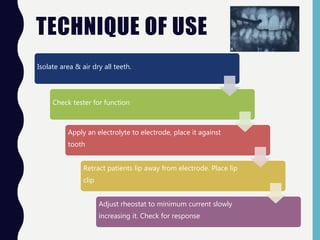
TECHNIQUE OF USE
Isolatearea & air dry all teeth.
Check tester for function
Apply an electrolyte to electrode, place it against
tooth
Retract patients lip away from electrode. Place lip
clip
Adjust rheostat to minimum current slowly
increasing it. Check for response
54.
FALSE RESPONSE
Patient relatedfactors
Tooth characteristics
Restored teeth
Supporting tissues
Apex maturation
Repeated trials
Psychological state
Physiological state
Failure to
complete the
circuit
Equipment
problems
Probe
placement
Interface
media
55.
FALSE POSITIVE &NEGATIVE
Necrotic pulp responds to testing.
Stimulation of adjacent teeth
The response of vital tissue in multirooted tooth with
pulp necrosis in one or more canals
Patient interpretation: subjectivity
Vital pulp that does not respond to
stimulation
Inadequate contact with the stimulus
Tooth calcification
Immature apical development
Traumatic injury
Subjective nature of the tests
Elderly patients – regressive neural changes
Analgesics for pain
Traumatic injury
56.
LIMITATIONS OF EPT
Noinformation on health status/ integrity
Unreliable for immature teeth
Not suitable with full coverage restorations
Chances of ventricular fibrillation
57.
LIMITATIONS
1. Subjective; measureonly nerve supply
2. Thermal tests: not effective in substantial secondary dentine
formation
3. Unreliability of tests: Immature apices, traumatic injuries, more
subjectivity in the young
4. No correlation with the histologic status
5. Difficult to administer & inconclusive in children
6. Weaker response- aged pulp
7. Extensive restorations, pulp recession, pulp calcification
8. Lack of reproducibility
58.
SAFETY CONCERNS
Zach etal. Increase in 11 degree C without cooling can damage pulp. Hence contact to be minimized
less than 5 secs.
Lutz et al carbon dioxide snow causes cracks. Later disproved by Peters et al & Fuss et al.
EPT of concern in patients with cardiac pace makers
59.
TEST CAVITY
Non localized,acute diffuse radiating pain
Definitive diagnosis: impossible
Cavity prepared in the tooth without anesthesia
Patient apprised of what to expect & how to respond
Young teeth: immature roots- invasive nature questioned
Unreliable; response even in necrotic pulp
Response unreliable: anxiety
Invasive & irreversible
No further information than thermal & EPT
Not justified in modern practice
60.
ANESTHETIC TEST
L/A: painfularea
Block/ infiltration/ intraosseous
Vague location of pain
Non odontogenic pain:Myocardial infarction
Differentiating between arches
PDL- identify source of pulpal pain.
61.
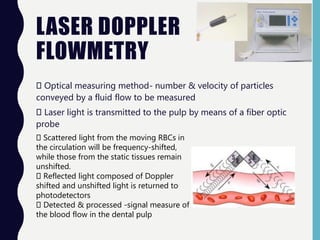
LASER DOPPLER
FLOWMETRY
Optical measuringmethod- number & velocity of particles
conveyed by a fluid flow to be measured
Laser light is transmitted to the pulp by means of a fiber optic
probe
Scattered light from the moving RBCs in
the circulation will be frequency-shifted,
while those from the static tissues remain
unshifted.
Reflected light composed of Doppler
shifted and unshifted light is returned to
photodetectors
Detected & processed -signal measure of
the blood flow in the dental pulp
62.
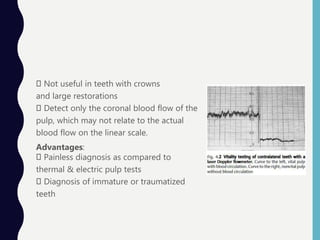
Not useful inteeth with crowns
and large restorations
Detect only the coronal blood flow of the
pulp, which may not relate to the actual
blood flow on the linear scale.
Advantages:
Painless diagnosis as compared to
thermal & electric pulp tests
Diagnosis of immature or traumatized
teeth
63.
PULSE OXIMETRY
Effective, objectiveoxygen saturation monitoring technique –
intravenous anesthesia
Consistently determined the level of blood oxygen saturation of
the pulp- pulp vitality testing
Correlation between
pulp and systemic
oxygen saturation
readings (Schnettler
Biox 3740 Oximeter
(Kahan et al 1996)
Custom-made Pulse
Oximeter sensor
holder (Gopikrishna et
al 2006)
64.
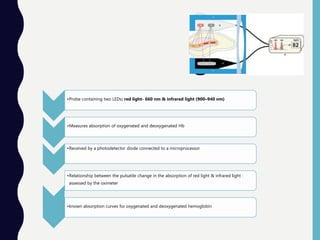
•Probe containing twoLEDs: red light- 660 nm & infrared light (900–940 nm)
•Measures absorption of oxygenated and deoxygenated Hb
•Received by a photodetector diode connected to a microprocessor
•Relationship between the pulsatile change in the absorption of red light & infrared light :
assessed by the oximeter
•known absorption curves for oxygenated and deoxygenated hemoglobin
65.
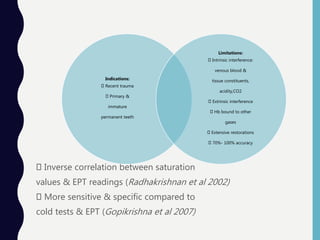
Inverse correlation betweensaturation
values & EPT readings (Radhakrishnan et al 2002)
More sensitive & specific compared to
cold tests & EPT (Gopikrishna et al 2007)
Indications:
Recent trauma
Primary &
immature
permanent teeth
Limitations:
Intrinsic interference:
venous blood &
tissue constituents,
acidity,CO2
Extrinsic interference
Hb bound to other
gases
Extensive restorations
70%- 100% accuracy
66.
DUAL WAVELENGTH
SPECTROPHOTOMETRY
Method independentof a pulsatile circulation
Measures oxygenation changes in the
capillary bed rather than in the supply vessels
Detects the presence or absence of
oxygenated blood at 760 nm and 850nm.
Advantage: Uses visible light that is filtered
and guided to the tooth by fibreoptics
67.
ULTRAVIOLET
LIGHT/FIBEROPTIC
FLUORESCENT SPECTROMETRY
Fluorescence
Vital teethfluoresce normally; necrotic & RCT teeth do not
Lighting in the operatory fully suppressed
Patient & staff wear suitable protective goggles
Fluorescence from the pulp –substantially lower than the
healthy and decayed dentin fluorescence.
Healthy and decayed dentin patterns differentiated
68.
PHOTOPLETHYSMOGRAPHY
Optical measurement technique: blood volume changes in
the microvascular bed of tissue.
Light source to illuminate the tissue & a photodetector to
measure the small variations in light intensity associated with
changes in perfusion
69.
TOOTH SURFACE
TEMPERATUREpulp circulationmaintains tooth temperature
Thermistor
Cholesteric crystals:10% solution in
chlorinated hydrocarbon
solvent(Howell et al)- non vital
Electronic
Thermography
Infrared sensor,control unit,thermal
image computer,software,color
monitor,printer
Differences in superficial areas not
sensitive
Hughes Probeye
4300 thermal
video
system
sensitive to measure 0.1oc
Patient temperature
Baseline temperature: follwed up
Patient is improving/ worsening
>1000oF : systemic response to
infection
70.
ULTRASOUND
Compliment conventional radiography
Highresolution, 3D images- inner macrostructure of the tooth
A transducer (a crystal containing probe), a coupling agent &
software
Detect cracks in a simulated human tooth
Detect vertical root fractures – vital & nonvital teeth
71.
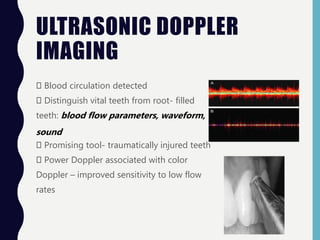
ULTRASONIC DOPPLER
IMAGING
Blood circulationdetected
Distinguish vital teeth from root- filled
teeth: blood flow parameters, waveform,
sound
Promising tool- traumatically injured teeth
Power Doppler associated with color
Doppler – improved sensitivity to low flow
rates
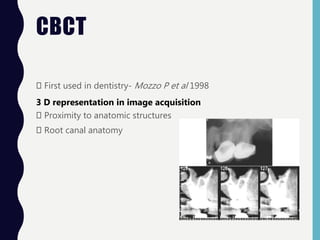
CBCT
First used indentistry- Mozzo P et al 1998
3 D representation in image acquisition
Proximity to anatomic structures
Root canal anatomy
76.
REFERENCESWeine F .6th ed. 2003.Endodontic therapy. Mosby publications
Ingle et al.6th ed. 2008..Endodontics.BC Decker Inc
Cohen’s Pathways of the Pulp- 10th ed
Grossman.13th ed.2015.Endodontic practice. Wolters kluver
Endodontics- Problem solving in Clinical practice- Pitt Ford
Practical Endodontics- A clinical guide. Bessner & Ferrigno
Pocket Atlas of Endodontics- Beer
H. Jafarzadeh & P. V. Abbott. Review of pulp sensibility tests.
Part I: general information and thermal tests. IEJ, 43, 738- 762,
2010
Yoon et al. JOE- Volume 36, No.3, March 2010
Jespersen et al. JOE- Volume 40, No.3, March 2014
77.
‘‘FOR I SEEKTHE TRUTH BY
WHICH NO MAN HAS EVER BEEN
HARMED.’’
—MARCUS AURELIUS,
MEDITATIONS VI. 21, 173 AD










































![endo diagnosis ppt friday.pptx [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/endodiagnosispptfriday-240220084902-bcb16ad0-thumbnail.jpg?width=640&height=640&fit=bounds)








































