Downloaded 218 times
![Sarantos Kaptanis [email_address] Airedale General Hospital Department of Surgery Teaching Session 27 August 2009](https://image.slidesharecdn.com/skaptanisvaricoseveins-12554111412036-phpapp03/85/Varicose-Veins-1-320.jpg)
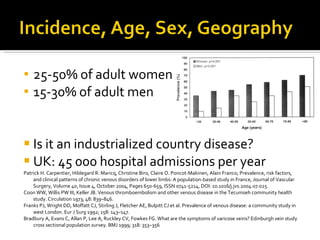

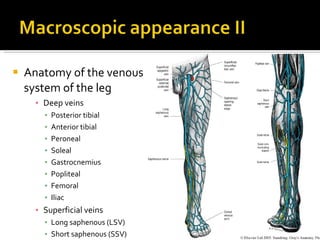





This document provides a summary of varicose veins including: - Incidence rates that are higher in women and industrialized countries - Risk factors such as family history, pregnancy, prolonged standing, and obesity - Presentation with dilated, tortuous veins and possible complications like eczema or ulcers - Examination techniques including looking for varicose veins while standing and using tests like cough impulse and Doppler ultrasound - Treatment options ranging from compression stockings and sclerotherapy to surgical procedures like vein stripping















































