Download to read offline

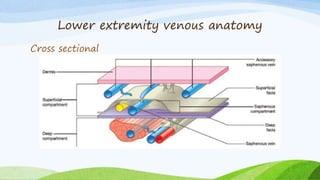
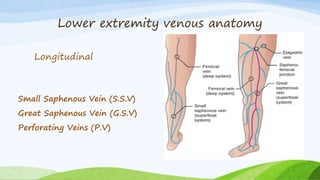
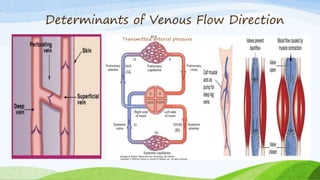
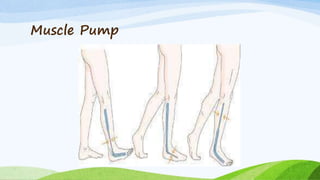
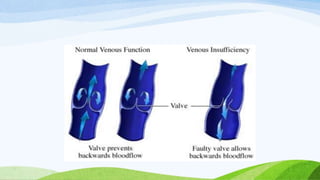



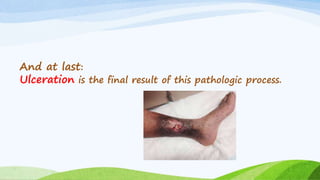









The document discusses chronic venous insufficiency (CVI) and its management, highlighting the anatomy and physiology of the venous system, as well as the pathophysiology, risk factors, and clinical manifestations of CVI. It emphasizes that reflux is a key factor in CVI, leading to symptoms such as edema and ulceration, while identifying diagnostic evaluations and treatment options including wound care, compression therapy, and surgical interventions. Successful management of CVI relies on addressing the root causes of reflux and employing effective compression therapy.



































































