Recommended

Recommended
More Related Content
What's hot
What's hot (20)
Similar to When Back Pain Leads to Posterior Leukoencephalopathy Syndrome
Similar to When Back Pain Leads to Posterior Leukoencephalopathy Syndrome (20)
More from mfabzak
Recently uploaded
Recently uploaded (20)
When Back Pain Leads to Posterior Leukoencephalopathy Syndrome
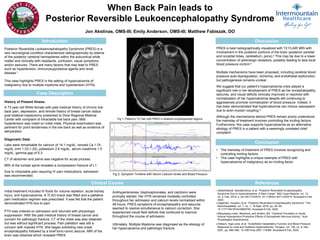
- 1. When Back Pain leads to Posterior Reversible Leukoencephalopathy Syndrome Jon Akstinas, OMS-III; Emily Anderson, OMS-III; Matthew Fabiszak, DO Introduction Posterior Reversible Leukoencephalopathy Syndrome (PRES) is a rare neurological condition characterized radiographically by edema of the posterior cerebral hemispheres within the subcortical white matter and clinically with headache, confusion, visual symptoms and/or seizures. There are many factors that may lead to PRES such as hypertension, immunosuppressive agents and renal disease.1 This case highlights PRES in the setting of hypercalcemia of malignancy due to multiple myeloma and hypertension (HTN). Clinical Course Case Description History of Present Illness: A 73 year old White female with past medical history of chronic low back pain, depression, and remote history of breast cancer status post bilateral mastectomy presented to Dixie Regional Medical Center with complaint of intractable low back pain. Mild hypertension was noted on initial vitals. Physical examination was pertinent for point tenderness in the low back as well as evidence of dehydration. Diagnostic Data: Labs were remarkable for calcium of 14.1 mg/dL, ionized Ca 1.74 mg/dL (nml 1.03-1.25), potassium 2.6 mg/dL, serum creatinine 1.5 mg/dL, gamma gap of 5.3. CT of abdomen and pelvis was negative for acute process. MRI of the lumbar spine revealed a compression fracture of L1. Due to intractable pain requiring IV pain medications, admission was recommended. Discussion PRES is best radiographically visualized with T2 FLAIR MRI with involvement in the posterior portions of the brain (posterior parietal and occipital lobes, cerebellum, pons).2 This may be due to a lower concentration of adrenergic receptors, possibly leading to less local blood pressure control.3 Multiple mechanisms have been proposed, including cerebral blood pressure auto-dysregulation, ischemia, and endothelial dysfunction, but pathogenesis remains unclear. We suggest that our patient’s hypercalcemia crisis played a significant role in her development of PRES as her encephalopathy, seizures, and visual deficits clinically improved or resolved with normalization of her hypercalcemia despite still continuing to aggressively promote normalization of blood pressure. Indeed, it has been demonstrated that hypercalcemia can induce vasospasm due to actin-myosin coupling.4 Although the mechanisms behind PRES remain poorly understood, the mainstay of treatment involves controlling the inciting factors. Furthermore, this case supports hypercalcemia as an alternative etiology of PRES in a patient with a seemingly unrelated chief complaint. Antihypertensives, bisphosphonates, and calcitonin were promptly started. Her HTN remained modestly controlled throughout her admission and calcium levels normalized within 48 hours. PRES symptoms of encephalopathy and seizures seemed to resolve simultaneous to calcium correction. She experienced visual field deficits that continued to improve throughout the course of admission. Ultimately, Multiple Myeloma was diagnosed as the etiology of her hypercalcemia and pathologic fracture. Fig 1: Patient’s T2 Flair with PRES in bilateral occipitoparietal regions. Conclusion • The mainstay of treatment of PRES involves recognizing and controlling inciting factors. • This case highlights a unique example of PRES with hypercalcemia of malignancy as an inciting factor. References 1.Bolanthakodi, Nandakrishna, et al. “Posterior Reversible Encephalopathy Syndrome Due to Hypercalcaemia: A Rare Cause.” BMJ Case Reports, vol. 12, no. 2, Feb. 2019, p. bcr-2017-223415, 10.1136/bcr-2017-223415. Accessed 9 Feb. 2020. 2.Algahtani, Hussein, et al. “Posterior Reversible Encephalopathy Syndrome.” The Neurohospitalist, vol. 7, no. 1, 18 Sept. 2016, pp. 24–29, 10.1177/1941874416665762. Accessed 8 Feb. 2020. 3.Beausang-Linder, Marianne, and Anders, Bill. “Cerebral Circulation in Acute Arterial Hypertension-Protective Effects of Sympathetic Nervous Activity.” Acta Physiologica Scandinavica, 4.Nilsson, Inga-Lena, et al. “Endothelial Vasodilatory Function and Blood Pressure Response to Local and Systemic Hypercalcemia.” Surgery, vol. 130, no. 6, Dec. 2001, pp. 986–990, 10.1067/msy.2001.118368. Accessed 9 Feb. 2020. Initial treatment included IV fluids for volume repletion, acute kidney injury, and hypercalcemia. A TLSO brace was fitted and a palliative pain medication regimen was prescribed. It was felt that the patient demonstrated HTN due to pain. PTH was ordered on admission and returned with physiologic suppression. With the past medical history of breast cancer and concern for pathologic fracture, CT of the chest was also obtained but was without significant process. Pain palliation was still a concern with marked HTN. She began exhibiting new onset encephalopathy followed by a brief tonic-clonic seizure. MRI of the brain was obtained which revealed PRES. Fig 2: Symptom Timeline with Serum Calcium levels and Blood Pressure Onset Encephalopathy and Seizures Resolved