Downloaded 322 times


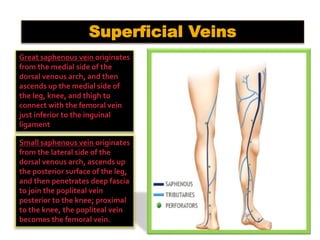
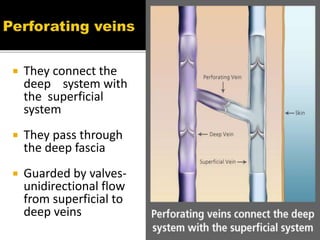
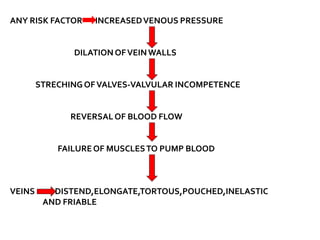
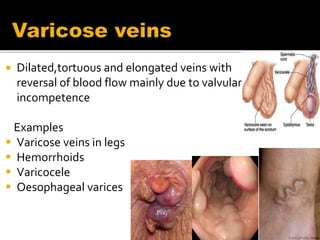





The document summarizes the venous drainage system of the lower extremity. It consists of deep, superficial, and perforating veins, all containing one-way valves. The great and small saphenous veins are the major superficial veins, draining into the femoral and popliteal veins respectively. Perforating veins connect the deep and superficial systems. Risk factors for varicose veins include increased venous pressure from factors like aging, genetics, pregnancy, and obesity. Varicose veins occur when valves become incompetent, causing reversed blood flow and vein dilation. Symptoms include aching pain and appearance of dilated, tortuous veins. Diagnosis involves physical exams and imaging tests. Treatment options are conservative compression or surgical procedures like vein


































































