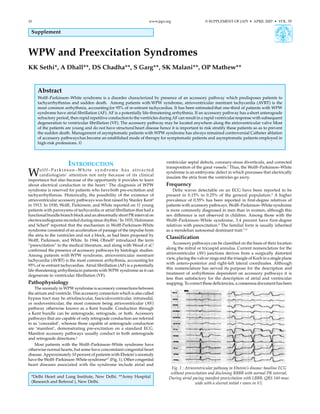
1. Wolff-Parkinson-White syndrome is characterized by an accessory pathway that predisposes patients to tachyarrhythmias and sudden death. Atrioventricular reentrant tachycardia is the most common arrhythmia in WPW syndrome patients.
2. Atrial fibrillation is a potentially life-threatening arrhythmia in WPW syndrome patients. Rapid conduction during AF can cause ventricular fibrillation.
3. Catheter ablation has become an established treatment for symptomatic WPW patients and asymptomatic patients in high-risk professions to prevent sudden death.
Cryptogenic stroke and PFO have always been a controversial topic with no closure trial in the past showing significant benefit from closing the PFO in preventing the recurrent stroke. Also thought to be due to imperfect definition of cryptogenic stroke which is evolving with drop in the fraction of patients from 20-40% in the past to very fewer numbers due to increased understanding of the mechanisms involved in acute stroke. Recent trials REDUCE and CLOSE targeted the niche population of PFO with moderate to large shunt and atrial septal aneurysm and showed benefit of closing PFO compared to the antiplatelet therapy alone but with the risk of A.fib, device and procedure related complications. This presentation is made in the Cerebrovascular center weekly conference at the Cleveland Clinic with my perspective after these current trials.
Cryptogenic stroke and PFO have always been a controversial topic with no closure trial in the past showing significant benefit from closing the PFO in preventing the recurrent stroke. Also thought to be due to imperfect definition of cryptogenic stroke which is evolving with drop in the fraction of patients from 20-40% in the past to very fewer numbers due to increased understanding of the mechanisms involved in acute stroke. Recent trials REDUCE and CLOSE targeted the niche population of PFO with moderate to large shunt and atrial septal aneurysm and showed benefit of closing PFO compared to the antiplatelet therapy alone but with the risk of A.fib, device and procedure related complications. This presentation is made in the Cerebrovascular center weekly conference at the Cleveland Clinic with my perspective after these current trials.
Natural history of common congenital heart diseasesRamachandra Barik
Most infants with ASDs are asymptomatic
They may present at 6 to 8 weeks of age with a soft systolic ejection murmur and possibly a fixed and widely split S2
CHF rare in the first decades of life but it can become common once the patient is older than 40 yrs
Definition of LVA Centerline analysis of RWMA on LV angio in 30º RAO shows hypocontractile segments moving more than 2 standard deviations out of normal range.
Powerpoint Presentation - exported from Keynote Mac presentation. Introduction to Cardiac Point of Care U/S. Talk was meant for Emergency Medicine Residents PG1-3 level. Modest tweaks of font and spacing required prior to your own use. Associated PDF file in original Keynote format.
Libro que analiza lo que solamente podemos alcanzar a percibir con la mirada interna, las fuerzas que en la gran mayoría de ocasiones pasan desapercibidas para nuestros sentidos pero que al mismo tiempo dan sustancia a esta realidad.
Divorce and marriages infographic by Alan Weiss Aussie Divorceaussiedivorce.com.au
Divorce is the legal term used to describe the formal dissolution of a marriage. A divorce may be granted by either the Family Court of Australia or the Federal Circuit’s Court. Generally, these courts will have jurisdiction over a divorce provided both parties are resident in Australia or have lived as husband and wife in Australia.
http://www.aussiedivorce.com.au/family-law/divorce-in-australia.php
Natural history of common congenital heart diseasesRamachandra Barik
Most infants with ASDs are asymptomatic
They may present at 6 to 8 weeks of age with a soft systolic ejection murmur and possibly a fixed and widely split S2
CHF rare in the first decades of life but it can become common once the patient is older than 40 yrs
Definition of LVA Centerline analysis of RWMA on LV angio in 30º RAO shows hypocontractile segments moving more than 2 standard deviations out of normal range.
Powerpoint Presentation - exported from Keynote Mac presentation. Introduction to Cardiac Point of Care U/S. Talk was meant for Emergency Medicine Residents PG1-3 level. Modest tweaks of font and spacing required prior to your own use. Associated PDF file in original Keynote format.
Libro que analiza lo que solamente podemos alcanzar a percibir con la mirada interna, las fuerzas que en la gran mayoría de ocasiones pasan desapercibidas para nuestros sentidos pero que al mismo tiempo dan sustancia a esta realidad.
Divorce and marriages infographic by Alan Weiss Aussie Divorceaussiedivorce.com.au
Divorce is the legal term used to describe the formal dissolution of a marriage. A divorce may be granted by either the Family Court of Australia or the Federal Circuit’s Court. Generally, these courts will have jurisdiction over a divorce provided both parties are resident in Australia or have lived as husband and wife in Australia.
http://www.aussiedivorce.com.au/family-law/divorce-in-australia.php
Engagement marketing is all about growing your business by allowing your audience and potential customers to interact with you and shape how they would like to communicate with you. Engagement marketing begins when an interested person takes an action to begin an interaction with you.
http://lawyersmarketingbyalanweiss.blogspot.com.au/2014/10/engagement-marketing-secret-to-aussie.html?view=magazine
http://www.aussiedivorce.com.au
Sexual assault occurs when a person is forced, coerced or tricked into sexual acts against their will or without their consent, or if a child or young person under 18 is exposed to sexual activities.
Sexual assault is a crime. Sexual assault is not the victim's fault.
Sexual assault can happen to anyone in our community. This includes people who are young or old, male or female, from any cultural background, wealthy or not so wealthy, married or not. Anyone can be a victim of sexual assault.
Most victims of sexual assault know the person who assaulted them, such as a family member or friend or someone from work, school, church or another social group. A person you don't know or have just met can commit sexual assault.
http://nsw.criminallegal.com.au/crimes/sexual-assault/
Wolff–Parkinson–White syndrome (WPW) is one of several disorders of the conduction system of the heart that are commonly referred to as pre-excitation syndromes. WPW is caused by the presence of an abnormal accessory electrical conduction pathway between the atria and the ventricles. Electrical signals travelling down this abnormal pathway (known as the bundle of Kent) may stimulate the ventricles to contract prematurely, resulting in a unique type of supraventricular tachycardia referred to as an atrioventricular reciprocating tachycardia.The incidence of WPW is between 0.1% and 0.3% in the general population.Sudden cardiac death in people with WPW is rare (incidence of less than 0.6%), and is usually caused by the propagation of an atrial tachydysrhythmia (rapid and abnormal heart rate) to the ventricles by the abnormal accessory pathway.
ECG localization of accessory pathways slideshareCardiology
This presentation is simplified view of accessory pathways in heart and their localization with help of algorithms and ECG examples. Try to read this PPT in power point to see full effects and animations.
Pre-excitation Syndromes is a group of ECG and Electrophysiological abnormalities in which
The atrial impulses are conducted partly or completely, PREMATURELY, to the ventricles via a mechanism other than the normal AV-node *
Associated with a wide array of tachycardias with both normal QRS and prolonged QRS durations
Ohnell described this phenomenon as the “concertina
effect,” in which the QRS complex morphologies from individual
patients with WPW pattern differ owing to variation in the degree
of ventricular excitation via the accessory pathway and AV node.
Recognizing the concertina effect in WPW pattern as normal
variation is important to prevent unnecessary diagnostic and
therapeutic interventions.
AV nodal reentrant tachycardia (AVNRT), or atrioventricular nodal reentrant tachycardia, is a type of tachycardia (fast rhythm) of the heart. It is a type of supraventricular tachycardia (SVT), meaning that it originates from a location within the heart above the bundle of His. AV nodal reentrant tachycardia is the most common regular supraventricular tachycardia. It is more common in women than men (approximately 75% of cases occur in females). The main symptom is palpitations. Treatment may be with specific physical maneuvers, medication, or, rarely, synchronized cardioversion. Frequent attacks may require radiofrequency ablation, in which the abnormally conducting tissue in the heart is destroyed.
AVNRT occurs when a reentry circuit forms within or just next to the atrioventricular node. The circuit usually involves two anatomical pathways: the fast pathway and the slow pathway, which are both in the right atrium. The slow pathway (which is usually targeted for ablation) is located inferior and slightly posterior to the AV node, often following the anterior margin of the coronary sinus. The fast pathway is usually located just superior and posterior to the AV node. These pathways are formed from tissue that behaves very much like the AV node, and some authors regard them as part of the AV node.
The fast and slow pathways should not be confused with the accessory pathways that give rise to Wolff-Parkinson-White syndrome (WPW syndrome) or atrioventricular reciprocating tachycardia (AVRT). In AVNRT, the fast and slow pathways are located within the right atrium close to or within the AV node and exhibit electrophysiologic properties similar to AV nodal tissue. Accessory pathways that give rise to WPW syndrome and AVRT are located in the atrioventricular valvular rings. They provide a direct connection between the atria and ventricles, and have electrophysiologic properties similar to ventricular myocardium.