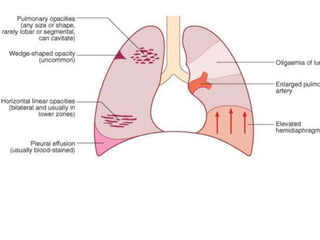
This document discusses venous thromboembolism (VTE), which includes deep vein thrombosis and pulmonary embolism. It notes that VTE can be caused by material traveling to the lungs through the pulmonary circulation. Risk factors include surgery, pregnancy, cardiorespiratory disease, lower limb problems, malignant disease, and immobility. Symptoms range from none for small embolisms to chest pain and circulatory collapse for large embolisms. Diagnosis involves assessing risk factors and alternative causes, with tests like chest x-rays, electrocardiograms, and D-dimer levels. Treatment is anticoagulation with heparin or warfarin and supportive measures.