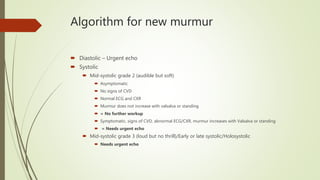
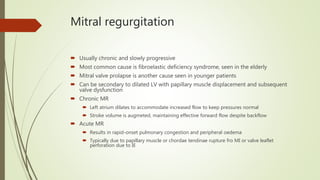
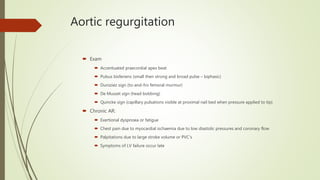
The document discusses valvular emergencies, highlighting the increased risk of death and stroke associated with new murmurs. It outlines the differential diagnosis for systolic and diastolic murmurs, emphasizing the need for urgent echocardiography in symptomatic cases while providing a grading system for murmurs and detailed clinical features for various valve disorders such as mitral stenosis, mitral regurgitation, and aortic stenosis. Management strategies, including medical treatment and surgical options, are also presented for each condition.