This document discusses systemic hypertension, including:
- Definitions of different classifications of hypertension according to WHO and AHA guidelines.
- Differences between hypertensive emergencies and urgencies.
- Common causes and clinical presentations of secondary hypertension.
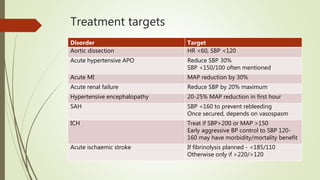
- Recommended treatment approaches for various hypertensive crises and emergencies, including targets for blood pressure reduction.
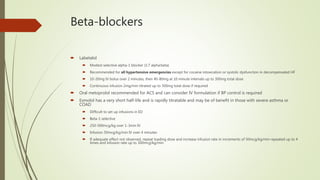
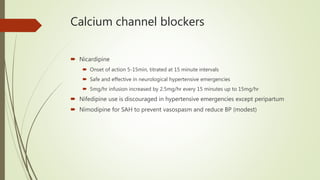
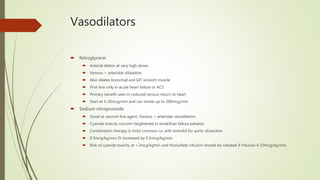
- Drugs commonly used to lower blood pressure such as labetalol, nicardipine, nitroglycerin, and sodium nitroprusside.



































![Hypertensive Crisis diagnosis treatment [1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypertensivecrisis1-241128145637-9d731b1a-thumbnail.jpg?width=640&height=640&fit=bounds)














































