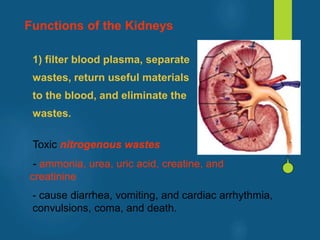
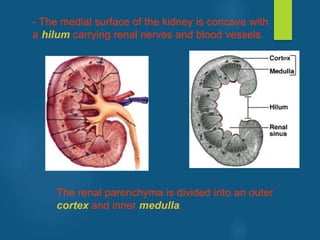
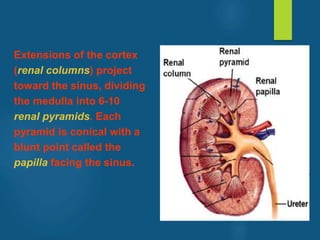
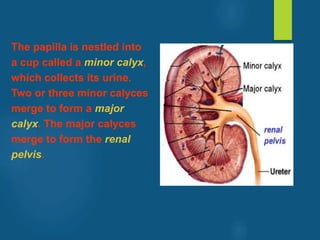
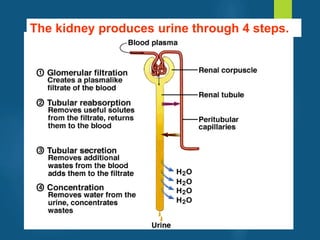
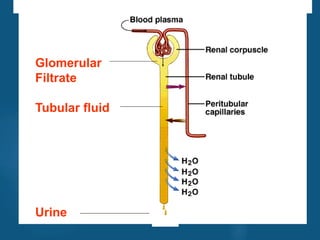

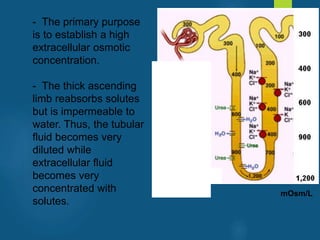
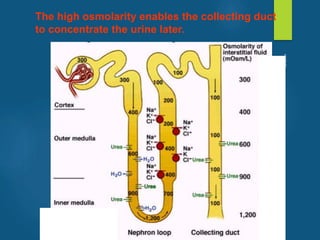
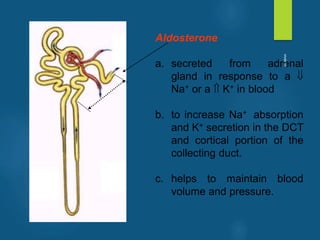
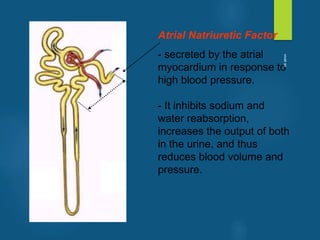
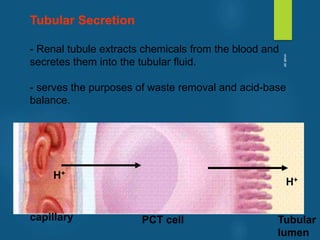
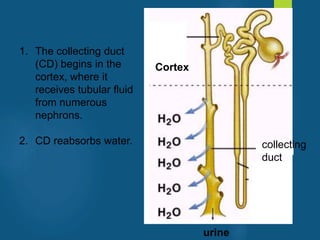
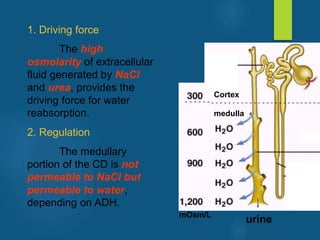
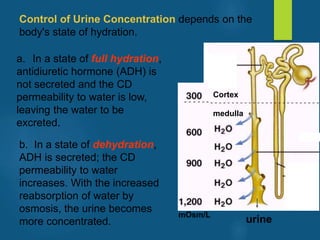
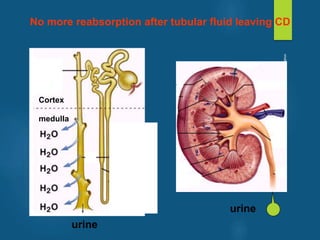
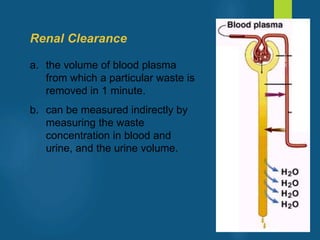
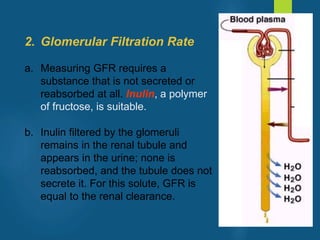

The document provides an overview of the urinary system, including its anatomy and functions. Some key points: - The kidneys filter blood to remove waste and regulate fluid balance. Each kidney contains around 1 million nephrons, the functional units that filter blood into urine. - The nephron is made up of blood vessels and tubules that work together to filter blood, reabsorb useful molecules, and secrete waste molecules into urine. - Urine is formed in four steps - glomerular filtration, tubular reabsorption, tubular secretion, and concentration by the collecting duct. Nearly all the filtrate is reabsorbed except for waste products. - Hormones











































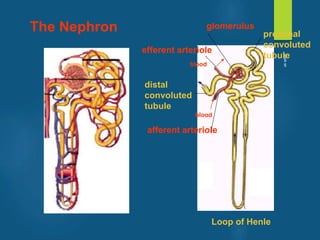
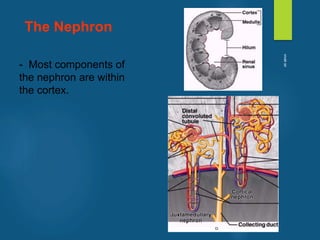
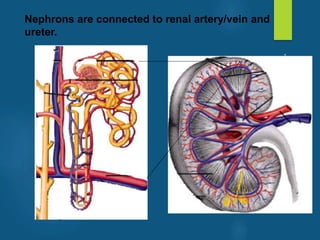
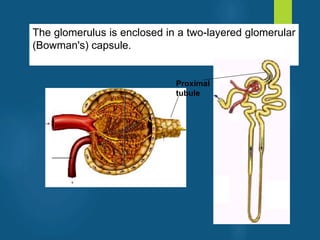
![26 [chapter 26 the urinary system]](https://cdn.slidesharecdn.com/ss_thumbnails/26chapter26theurinarysystem-170828044011-thumbnail.jpg?width=640&height=640&fit=bounds)









































