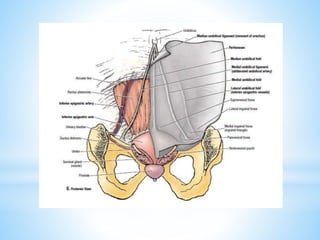
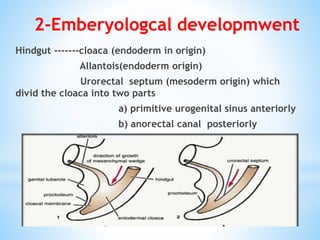
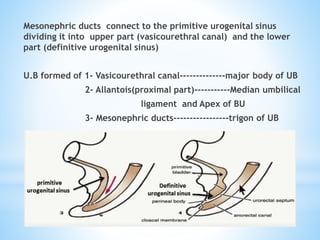
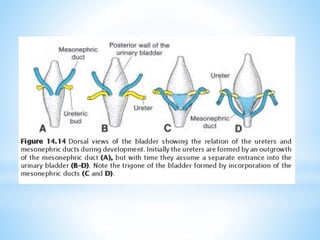
The document provides a comprehensive overview of urinary bladder (u.b) anatomy, embryological development, trauma types, clinical signs, imaging, management, and complications. It details the bladder's anatomy, including its positioning and relations, as well as various trauma mechanisms and classifications. The document concludes with management strategies for bladder injuries and potential complications that may arise from such injuries.