Learning objectives
1. Outlinethe common URTIs
2. Describe the etiology and pathophysiology of common
upper respiratory tract infections
3. Describe clinical manifestations of common upper
respiratory tract infections
4. Describe the complications of common upper respiratory
tract infections
5. Describe the nursing management of patients with
common upper respiratory tract infections
3.
Overview of theupper respiratory tract
Structures of the upper respiratory tract include:
• the nose,
• the nasal cavity,
•pharynx,
•epiglottis,
•Larynx
• trachea.
4.
Key features liableto pathogen infestation include:
Nasal mucosa: a sticky mucous membrane that lines
the nasal cavity and traps foreign particles
Para nasal sinuses:
mucosal-lined, air filled cavities in cranial bones
(frontal, ethmoidal, sphenoidal & maxillary bones)
that surround the nasal cavity; secrete mucus that
passes to the back of the nose to moisten the inhaled
air.
Pharynx or throat
5.
Overview of upperrespiratory tract infections
(URI)
• Represents the most common acute illness evaluated in the
outpatient settings.
• Range from the common cold—typically a mild, self-limited
ailment to life-threatening illnesses such as epiglottitis.
• Viruses account for most URIs
• Appropriate management of URI may consist of
reassurance, education, and instructions for symptomatic
home treatment
6.
Definition of commonURIs
• Rhinitis: Inflammation of the nasal mucosa
• Sinusitis: Inflammation of the paranasal sinuses, including
frontal, ethmoid, maxillary, and sphenoid
• Influenza (Flu) Generalized, acute, febrile, viral disease
associated with upper and lower respiratory infections
• Nasopharyngitis (rhinopharyngitis or the common cold):
Inflammation of the nares, pharynx, tonsils
7.
Definition of commonURIs CTs
•Pharyngitis: Inflammation of the pharynx,
•Epiglottitis (supraglottitis): Inflammation of the
superior portion of the larynx and supraglottic area
•Laryngitis: Inflammation of the larynx
•Laryngotracheitis: Inflammation of the larynx &
trachea.
•Tracheitis: Inflammation of the trachea
8.
The common occurringupper respiratory
conditions
• Rhinitis
• Influenza
• Sinusitis
9.
The common occurringupper respiratory
conditions CTs…,
Rhinitis
• Inflammation of the nasal mucosa
• Can be allergic or viral in origin
Allergic Rhinitis
• Most often, a reaction of the nasal mucosa to a specific antigen
• Caused by allergy to pollens from trees, flowers, crops
• Has therefore a seasonal trend
10.
Rhinitis CTs
AcuteViral rhinitis
• Also referred to as common cold
• Caused by virus that invade the upper respiratory tract
• Highly infectious condition spread by air born droplets
• Most prevalent in winter months
• Can be aggravated by chills, fatigue, emotional stress
• When uncomplicated, it is a self-resolving condition hence ABs are
not necessary.
11.
Rhinitis CTs
Pathophysiology
• Invasionof the nasal mucosal by the causative agent induces
inflammatory rxn
• There is also leukocytes infiltration and tissue edema because of
capillary permeability and vasodilation.
• This inflammatory response may be confined to the nasal
membranes or spread to regions where the nasal mucosa extends:
(nasolacrimal/tear ducts, paranasal sinuses, oropharynx)
• Can also progress to the chest as the nasal mucosal is continuous
with the respiratory tract
Clinical manifestations ofrhinitis cts…,
•Ocular manifestations may include profuse
tearing, bilateral conjuctival edema
•When inflammatory responses extend to the
Para nasal sinuses, the air in the sinuses gets
absorbed resulting into feeling of partial vacuum
and sinus headache localized over the inflamed
regions
14.
Clinical manifestations ofrhinitis CTs
Extension of the inflammation to the oropharynx may
present with:
• Cough
• Hoarseness of voice
• Snoring
• Recurrent need to clear the throat
Decreased hearing, a sensation of fullness or popping in the
ears may be evident of eustachian tube involvement
15.
Complications of rhinitis
Mostlylinked with acute viral rhinitis and these
include:
•Sinusitis
•Otitis media
•Pharyngitis
•Tonsillitis
•Lung infections
16.
Diagnostic approaches
Mostly through:
•Hx taking: ( onset, aggravating factors: environmental related)
• Physical examination; routine head to toe exam with focus on the
general appearance & presentation of the clinical manifestations; the
goal being to asses extent and severity of organ involvement
Ocular involvement
Extent of nasal membrane inflammation
Oropharyngeal involvement
• Check of vital signs
• Review of lab results (FBC;)
17.
Treatment plan forrhinitis
•Aimed at blocking symptoms
•Maintaining optimal functioning.
•Prevent complications
18.
Key rx approachesinclude:
Environmental control: identifying and avoiding
triggers of the allergic rxns (allergic rhinitis)
Drug therapy: ( anti-histamines and
decongestants;eg phenylephrine o.25%, 2 drops in
each nostril); to manage symptoms: reading
assignment on other specific drugs in use
Supportive care: Increase fluid intake to liquefy
secretions & counter loss from obligatory mouth
breathing
19.
Nursing management ofpatients with rhinitis
•Nursing interventions are directed towards relief
of uncomfortable symptoms
•Increasing fluid intake is key to aid in liquefying
secretions
•Administering the ordered antihistamines and
decongestants helps to reduce severity of
symptoms
20.
Nursing management ofpatients with Rhinitis
CTs
Nursing diagnoses
• Defined according to specific patient presentation
• Obvious ones could be:
Ineffective breathing pattern……..; further defined in the
context of the presence of the following: (Obligatory mouth
breathing, dyspnea, snoring)
Eg: Ineffective breathing pattern related to nasal mucosal
membrane congestion secondary to the disease
process(inflammation) evidenced by obligatory mouth
breathing
21.
Nursing diagnosis CTs
Goalof care: Patient to breath at ease and through the nostrils 1 hour
after nursing interventions.(specify the easiness of the breathing)
Nursing interventions:
• Explain condition to patient to gain cooperation
• Elevate head of bed to 45 degrees to facilitate mucous drainage
• Assess environment for presence of offending allergen and remove it
if possible
• Administer the prescribed decongestant( specify name, dose etc etc)
• Emphasize importance of nasal breathing
22.
Nursing diagnoses CTs
Othernursing diagnoses to address the following:
•Fluid intake
•Nutrition
•Health maintenance (need to prevent
symptoms)
•Susceptibility to infections like infective otitis
media, infective conjunctivitis
23.
Patient education
Key areasto include:
• Disease process; reinforce the concept of self-care and self
management of the disease
• Environmental control measures and patient`s
responsibilities
• Medications in use, side effects and rationale for use of such
medications
• Importance of monitoring the symptoms, response to
therapies, any difficulties, new symptoms etc etc
24.
Influenza
Disease overview
• Alsotermed as Flu
• Generalized, acute, febrile, viral disease associated with
upper and lower respiratory infections
• There are 3 known groups of flu viruses ( A, B & C), all with
many mutagenic strains; ie; have a remarkable ability to
change over time; rendering it a widespread disease
• C believed to have little pathogenic potential.
25.
Pathophysiology
• Flu virusesare inhaled in mucus droplets from infected
persons
• These then penetrate the surface of upper resp tract
mucosal cells causing cell lysis and destruction of the ciliated
epithelium
• This compromises viscosity of mucosa which facilitate spread
of virus containing exudate to the lower resp tract
• An interstitial inflammation and necrosis of the bronchiolar
and alveolar result, filling the alveoli with an exudate
containing leukocytes, erythrocytes
26.
Pathophysiology CTs
• Regenerationof epithelium slowly begins after 5th
day of the viral
infestation reaching maximum within 9 – 15 days; at which time
mucous production and cilia begin to appear.
• Before complete regeneration, the compromised epithelium is prone
to bacterial invasion and this can result into pneumonia
• If virus specific antibodies are adequate, the initial viral invasion can
be aborted at the port of entry
• The disease is usually self limiting; acute symptoms last 2 – 7 days and
are followed by convalescent period of about 1 wk
27.
Clinical manifestation
Onset usuallyabrupt and characterized by:
• fever,
• cough,
• headache,
• sore throat
If uncomplicated, symptoms may subside within 7 days
Complications
Mostly pneumonia
28.
Diagnostic approaches
• Hxtaking:
Hx of having travelled to flu prone regions
Sudden onset fever which rises and falls
Hx of general body pains, running nose, cough, sore throat
• Routine physical examination:
Check vital signs: high temp, increased resp rate
Check for conjunctivitis, erythema of soft palate
• Review lab investigation results(FBC, sputum culture)
29.
Treatment Plan
•Antipyretic forfever: ASA 600 mgs tds,
•Decongestants for nasal congestion eg
phenylephrine o.25%, 2 drops in each nostril
may be prescribed
•Increase in fluid intake
•Adequate rest
30.
Nursing management
•Primary goalsof nursing care are directed
at:
Relief of symptoms
Prevention of secondary infection:
• Disease is highly contagious hence
adherence to standard IP remains key
31.
Nursing management CTs
•Nursing diagnoses are patient specific and commonly with regard to:
Ineffective airway clearance
Potential for fluid deficit
Activity intolerance
Susceptibility to infection; pneumonia
Altered comfort
Transmission trend of the disease: highly infectious condition
32.
Patient education
Key Infoto include:
•Bed rest during acute phase
•Need for isolation
•Force fluid intake
•Alertness to symptoms of secondary
infection
33.
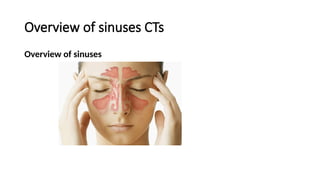
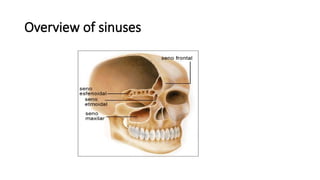
Sinusitis
Overview of sinuses
•Sinusesare air filled spaces in the skull and facial
bones.
•Make up the upper part of the respiratory tract from
the nose into the throat.
•Are located in the forehead (frontal sinuses), inside the
cheekbones (maxillary sinuses), and behind the nose
(ethmoid and sphenoid sinuses).
Sinusitis
Disease overview
• Aninflammatory process that produce changes in the mucosa of the
sinus (Inflammation of the tissues lining the sinuses)
• Can be caused by bacterial, viral or allergic conditions
• Frequently follows a common cold as infection spread from the nasal
cavity to the sinus.
• Forceful nasal blowing can also force infected materials into the
sinuses
• Swimming and diving can also cause acute onset of sinusitis
37.
Pathophysiology
• The nasalmucosa extend to the paranasal sinuses
• Therefore nasal cavity infections spread to these sinuses causing
sinusitis (inflamed sinuses)
• When infected materials block the passageways connecting the sinuses
to the nasal cavity, the air in the sinuses gets absorbed; resulting into a
partial vacuum and sinus headache localized over the inflamed area.
• With repeated attacks or infections remain unresolved/treated, the
mucosal lining of the sinus may become permanently damaged leading
to chronic suppurative sinusitis characterized by continued purulent
nasal discharge
38.
Clinical manifestation ofsinusitis
•Pain/pressure on the affected site/sinus
•Purulent nasal discharge
•Nasal congestion & obstruction
•Fever, general malaise
39.
Treatment plan forsinusitis
Use of nasal Decongestants
• Nasal sprays and nasal decongestants can be used for relief of the symptoms of acute
sinusitis.
• These medications help shrink the inflamed tissues and allow secretions and air to pass
through more easily.
• Over-the-counter nasal spray decongestants should only be used for a maximum of
three days.
• Prolonged use can cause tissues to become more inflamed and lead to a disorder called
rhinitis medicamentosa.
• Consult the doctor before using any drugs to treat sinusitis.
• Combinations of oral medications and nasal anti-inflammatories may be better options.
40.
Treatment plan CTs
•Use of antibiotics Usually Unnecessary
• Most cases of sinusitis are triggered by viruses such as the common cold
virus hence can not respond to antibiotics.
• Antibiotics should only be used in cases of sinusitis where a bacteria
pathogen is suspected and documented by a culture of the mucus from
your sinuses.
• Home remedies can help relieve some symptoms of sinusitis. (Breathing
in warm humidified air can help decrease symptoms of sinusitis.)
• If symptoms are due to allergies, over-the-counter antihistamines may
help.
41.
Nursing management
•Assessment approach;similar to above conditions
•Nursing diagnoses may include issues of:
Alteration in comfort
Sensory perceptual alteration: olfactory
Sleep pattern disturbances
Compromised breathing pattern
42.
Nursing interventions
May include:
•Bed rest
• Elevating head of bed to promote drainage of secretions
• Applying warm compresses prn for pain relief
• Administering the ordered analgesics,, antihistamines, Abs as may be
ordered
• IEC on self care and management of the condition
43.
IEC
Sinusitis Prevention
• Sinusitismay not be completely avoided; but there are ways to
prevent it in some cases:
Avoid smoking.
Avoid dry environments
Use a humidifier when needed
Drink plenty of fluids
Seek treatment for chronic allergies that can trigger sinus
inflammation
Key issues onURTIs
•URIs involve direct invasion of the mucosa lining
the upper airway.
•Bacterial/viral inoculation occurs when a person
directly inhales respiratory droplets from an
infected person who is coughing or sneezing.
46.
Key issues cts
Afterinoculation, viruses and bacteria encounter several barriers ( physical,
mechanical, humoral, and cellular immune defences):
• Hair lining the nose filters and traps some pathogens
• Mucus coats much of the upper respiratory tract, trapping potential
invaders
• The angle resulting from the junction of the posterior nose to the pharynx
causes large particles to impinge on the back of the throat
• Ciliated cells lower in the respiratory tract trap and transport pathogens
up to the pharynx; from there they are swallowed into the stomach
47.
Key issues CTs
•Adenoidsand tonsils contain immune cells that
respond to pathogens.
•Antigen/antibody rxns act to reduce infections
throughout the entire respiratory tract.
• Resident and recruited macrophages, monocytes,
neutrophils, and eosinophils coordinate to engulf and
destroy invaders.
48.
Key issues CTs
•A host of inflammatory cytokines mediates the immune response to
invading pathogens.
• Normal nasopharyngeal flora, including various staphylococcal and
streptococcal species, help to defend against potential pathogens.
Note:
Patients with suboptimal humoral and phagocytic immune function are
at increased risk for contracting URI, and they are at increased risk for
a severe or prolonged course of disease.
Inflammation (chronic or acute) from allergy predisposes individuals to
URI.






























![MANAGEMNT OF JAUNDICE FOR NURSING STUDENTSt[1].ppt](https://cdn.slidesharecdn.com/ss_thumbnails/jaundiceeditedfor2024cohort1-250318173231-642cf8e8-thumbnail.jpg?width=640&height=640&fit=bounds)
![Simulation based learning _Rev[1].ppt JOAB.ppt](https://cdn.slidesharecdn.com/ss_thumbnails/emamatiyafinalrev1-250309104337-a8877e76-thumbnail.jpg?width=640&height=640&fit=bounds)
![INTER-PERSONAL COMMUNICATION IN NURSING [1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/inter-communication1-250309103945-e946794c-thumbnail.jpg?width=640&height=640&fit=bounds)
![20971INTRODUCTION_TO_HIV&AIDS for nursing students[1].ppt](https://cdn.slidesharecdn.com/ss_thumbnails/20971introductiontohivaids1-250225134220-578a1188-thumbnail.jpg?width=640&height=640&fit=bounds)

![4. EDUCATIONAL PSYCHOLOGY EDITED[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/4-250224085157-3c676047-thumbnail.jpg?width=640&height=640&fit=bounds)
![The Immune system edited for 2024 cohort[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/theimmunesystemeditedfor2024cohort1-250224085036-4b3e6a28-thumbnail.jpg?width=640&height=640&fit=bounds)



![Pneumocystis_jirovecii_pneumonia[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/malamulo-pneumocystisjiroveciipneumonia1-241127111242-957cc6eb-thumbnail.jpg?width=640&height=640&fit=bounds)
![management of Chest_trauma for nursing [1].ppt](https://cdn.slidesharecdn.com/ss_thumbnails/malamulochesttrauma1-241127110255-71befbaa-thumbnail.jpg?width=640&height=640&fit=bounds)
![Chest_trauma types and management[1].ppt](https://cdn.slidesharecdn.com/ss_thumbnails/malamulochesttrauma1-241126062258-4b388e87-thumbnail.jpg?width=640&height=640&fit=bounds)
![ASTHMA_IN_CHILDREN for NURSING STUDENT[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/malamuloasthmainchildren1-241125202930-914bc525-thumbnail.jpg?width=640&height=640&fit=bounds)
![Acute Respiratory Infection Guidelines(ARI)__PRESENTATION[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/aripresentation1-241114171345-63d1411f-thumbnail.jpg?width=640&height=640&fit=bounds)
![Acute Respiratory Infections(ARI)__PRESENTATION[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/aripresentation1-241020112302-e350d353-thumbnail.jpg?width=640&height=640&fit=bounds)
![ECTOPIC_PREGNANCY_disorders of reproductive organs_1_(3)[1].ppt](https://cdn.slidesharecdn.com/ss_thumbnails/ectopicpregnancyupg131-241020092422-a0e8252f-thumbnail.jpg?width=640&height=640&fit=bounds)
![BURNS assessment and management_GRP_1_PPT[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/burnsgrp1ppt1-241020072724-5845af38-thumbnail.jpg?width=640&height=640&fit=bounds)
![Integrated Management -IMNCI_case_management_process[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/imncicasemanagementprocess1-241018200546-4cf422ad-thumbnail.jpg?width=640&height=640&fit=bounds)





![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)













