Fluid, Electrolyte and
Acid-base balance and
disorders
Medical Surgical nursing I
2024 cohort
17th
FEBRUARY 2025
By D. Kamalizeni
1
2.
2
Learning Objectives
(Refer tocontent of similar nature covered
in Biochemistry, Biophysiscs and HAP)
•Describe an overview of the fluid,
electrolyte and acid base balance in the
body.
•Describe the common alterations in fluid
and electrolyte balance
3.
Learning Objectives/Outcomes
CTs…..,
• Describethe assessment parameters for the
client with potential or actual fluid,
electrolyte and acid-base imbalance.
• Plan appropriate care for patients to
promote fluid, electrolyte and acid-base
balance
3
4.
Overview of fluidand electrolytes
balance in the body (revision)
Fluids constitute about 50 to +60% of the body
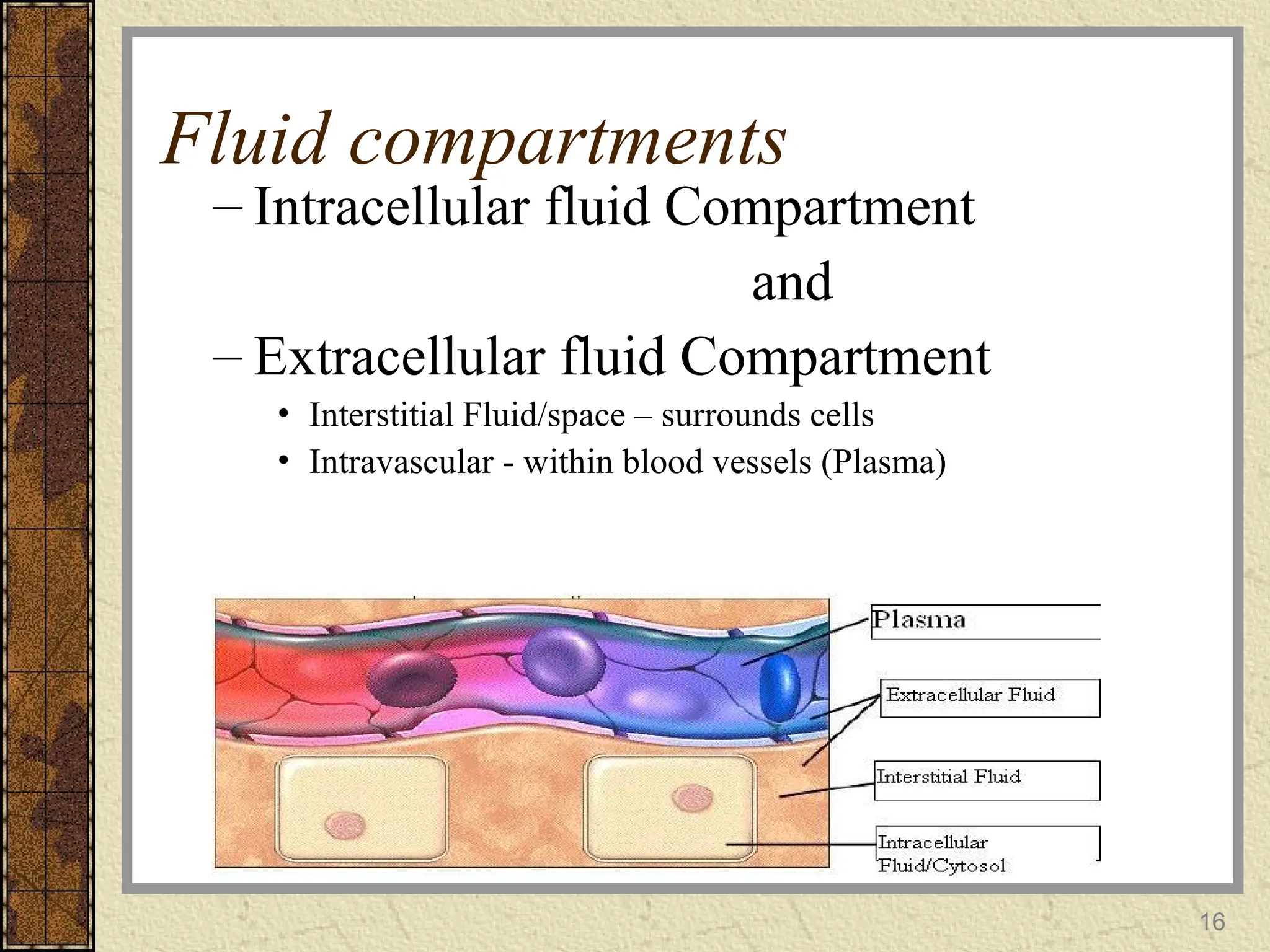
Fluids occupy 2 main compartments in the
body: Intracellular fluid (ICF);(2/3) and
Extracellular (ECF);(1/3)
Body fluids serve as universal solvents for
varied solutes broadly classified as electrolytes
and non-electrolytes and balance of these is a
must for health living
4
5.
Overview of electrolytesand non-
electrolytes
Electrolytes:
•Substances that dissociate/split into charged
particles(ions) when put in a solution; eg,
Sodium Chloride, Calcium Carbonate,
Potassium Chloride
•Ions are electrically charged particles:
•Can therefore conduct electrical current hence
are called electrolytes
5
6.
Electrolytes CTs….,
• Intheir ionized forms, some of these elements
play NB roles in the body:
Sodium maintains water balance,
Potassium and Calcium are necessary for nerve
impulse conduction, muscle contraction
• Composition of the electrolytes and
concentration of specific ions varies btn ICF &
ECF
6
7.
Overview of electrolytesand non-
electrolytes CTs
Non-electrolytes:
•Substances which do not dissociate into ions
when put in a solution
•Have bonds that prevent them from
dissociating when put in a solution
•No electrically charged species are created
when they dissolve in water; Eg glucose , urea
7
8.
Overview of Acidsand Bases
Are also electrolytes; they ionize and dissociate
in water
Acids
Substances that release hydrogen ions;
Also called proton donors
When dissolved in water, they release hydrogen
ions (protons) and anions, eg include;
Hydrochloric acid (HCL)
8
9.
Acids/bases CTs
The concentrationof the protons (hydrogen
ions) determines the acidity of a solution
Bases
• Substances that take up hydrogen ions, ie,
Proton acceptors, eg, Sodium Hydroxide
(NaOH)
• If this dissolves in water, it dissociates and
liberates hydroxyl ions and Sodium ions
9
10.
Acids/bases CTs
The hydroxylion then binds to (accepts) a
proton (hydrogen ion) present in the
solution
The rxn above produces water and
simultaneously reduces the acidity
(hydrogen ion concentration) in the solution
10
11.
pH and acidbase concentration)
The more hydrogen ions in a solution, the more
acidic the solution is.
Conversely, the greater the concentration of
hydroxyl ions, the lower the concentration of
hydrogen ions; the more basic or alkaline the
solution becomes
The relative concentration of hydrogen ions in
various body fluids is measured in a concentration
units called `pH units`
11
12.
The pH scale
Devisedby a Danish biochemist in the 1909
The scale runs from 1 to 14
At pH 7, the solution is neutral; neither acidic nor
basic; (hydrogen ions = hydroxyl ions) eg, pure water
Solution below pH 7 is acidic; (hydrogen ions
outnumber hydroxyl ions)
That above pH 7 are alkaline ( hydrogen ions are
decreasing)
12
13.
Balance
Balance is thestate of equilibrium (Stability),
where waste and excess products are efficiently
removed and necessary nutrients are always
available.
Intake of fluids = fluids excreted from body in
human homoeostatic state. Thereby maintaining
optimal hydration
In order to maintain homeostasis, fluid, electrolyte,
and acid/base levels must remain nearly constant
within their normal limits.
13
14.
Balance CTs…..,
In nursing,fluid balance refers to procedure
of measuring fluid input and output to
determine fluid need
14
15.
Importance of bodyfluids
Fluid essential to life and vital for:
– Controlling body temp
– Delivery of nutrients and gases to cells
– Removal of waste
– Acid – base balance
– Maintenance of cellular shape
15
Electrolyte composition influid
compartments
Each fluid compartment has a distinctive
pattern of concentration of the
electrolytes/nonelectrolytes
ICF contain small amounts of sodium and
chloride ions in contrast to ECF, plasma has
high protein content
17
18.
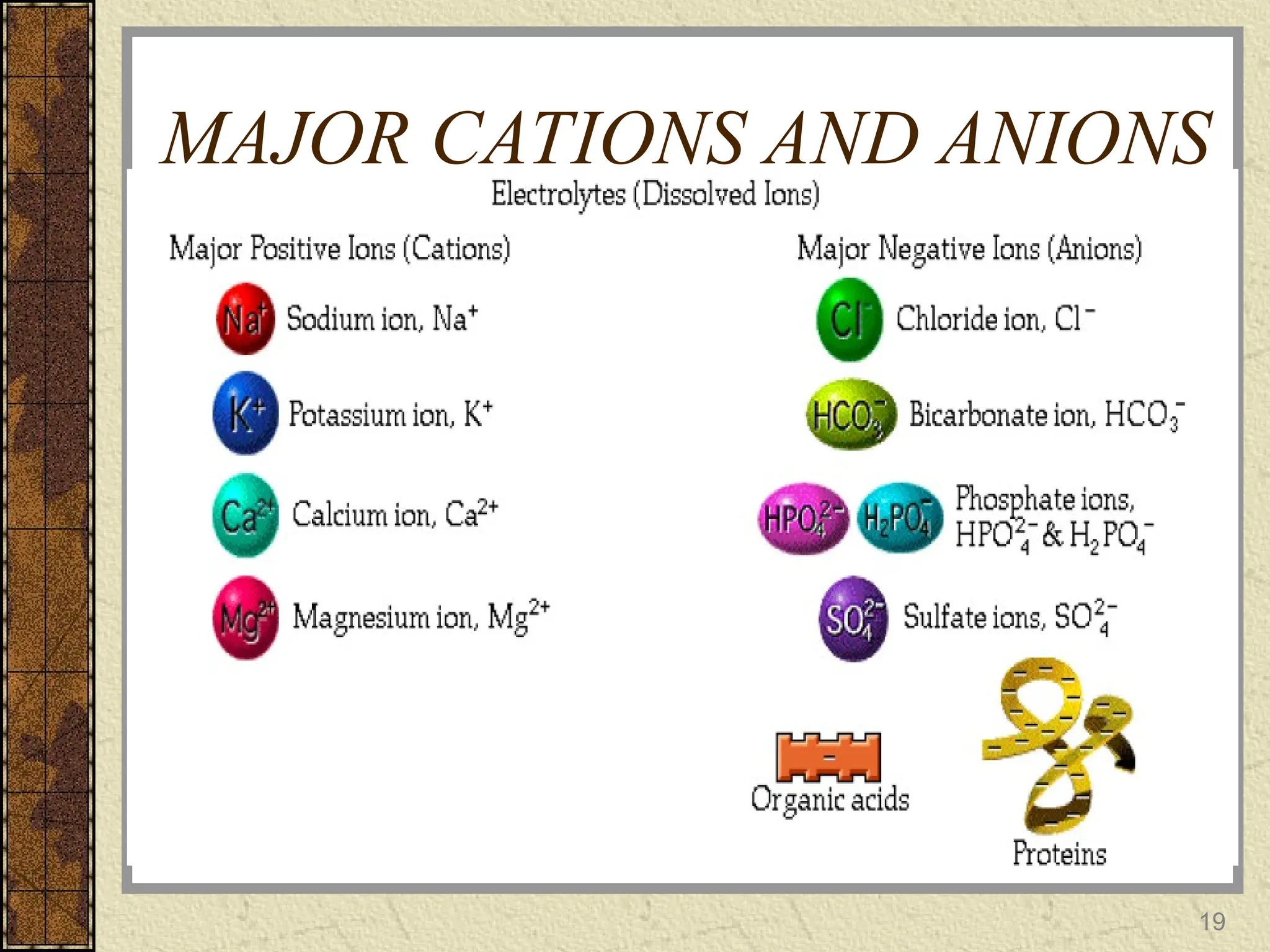
Electrolyte Balance
Refers tokeeping the concentration of each
electrolyte within normal limits
The most important electrolytes for body
function are Na+
,K+
,Ca2+
and Mg2+
,Cl-
,
Phosphate, sulphate and bicarbonate are
important as well.
Concentrations are different in the ICF and
ECF.
18
TRANSPORT AND MOVEMENT
OFWATER AND SOLUTES
Read on:
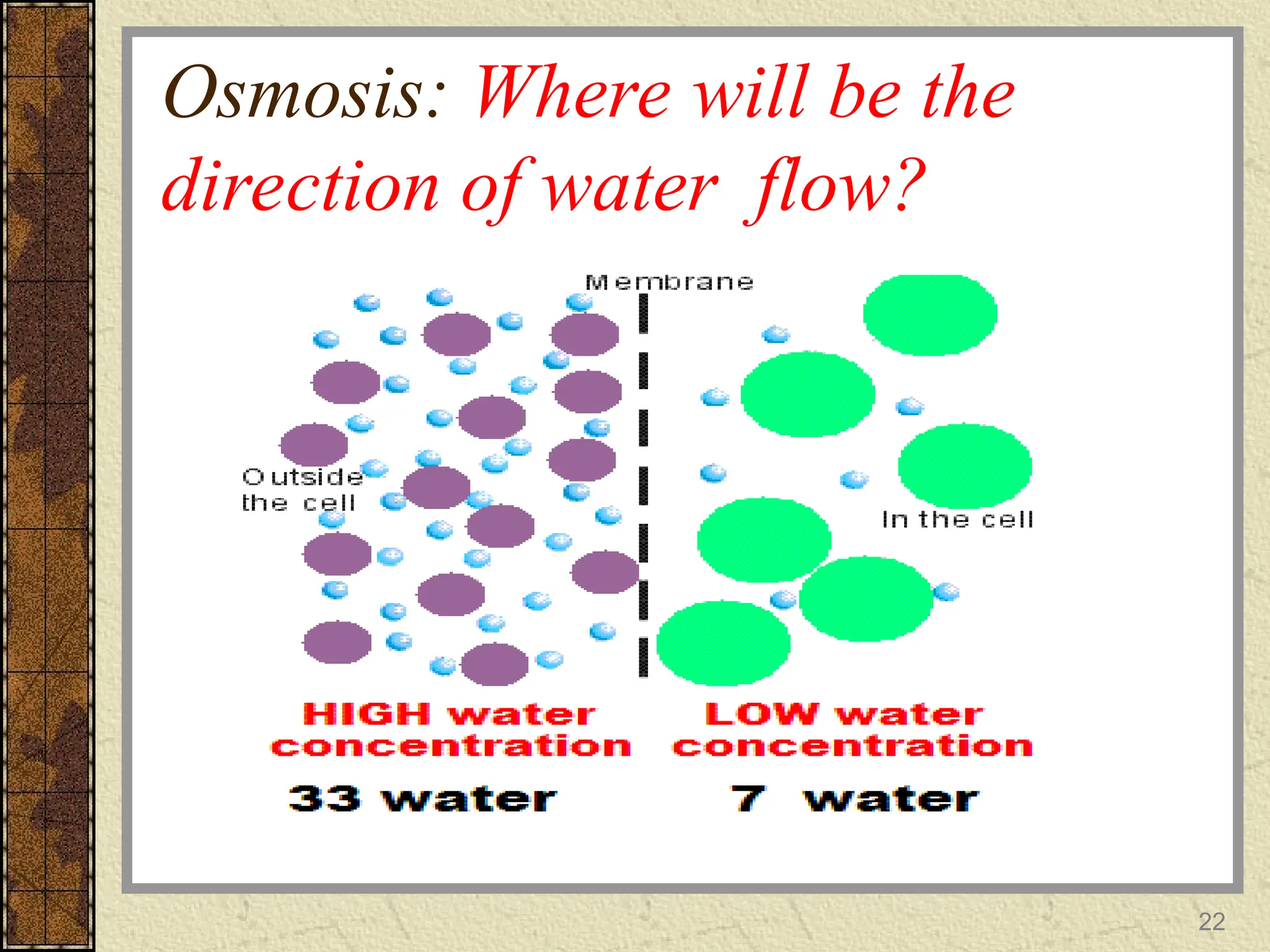
OSMOSIS
passage of a solvent through a membrane from
a dilute solution to a more concentrated one)
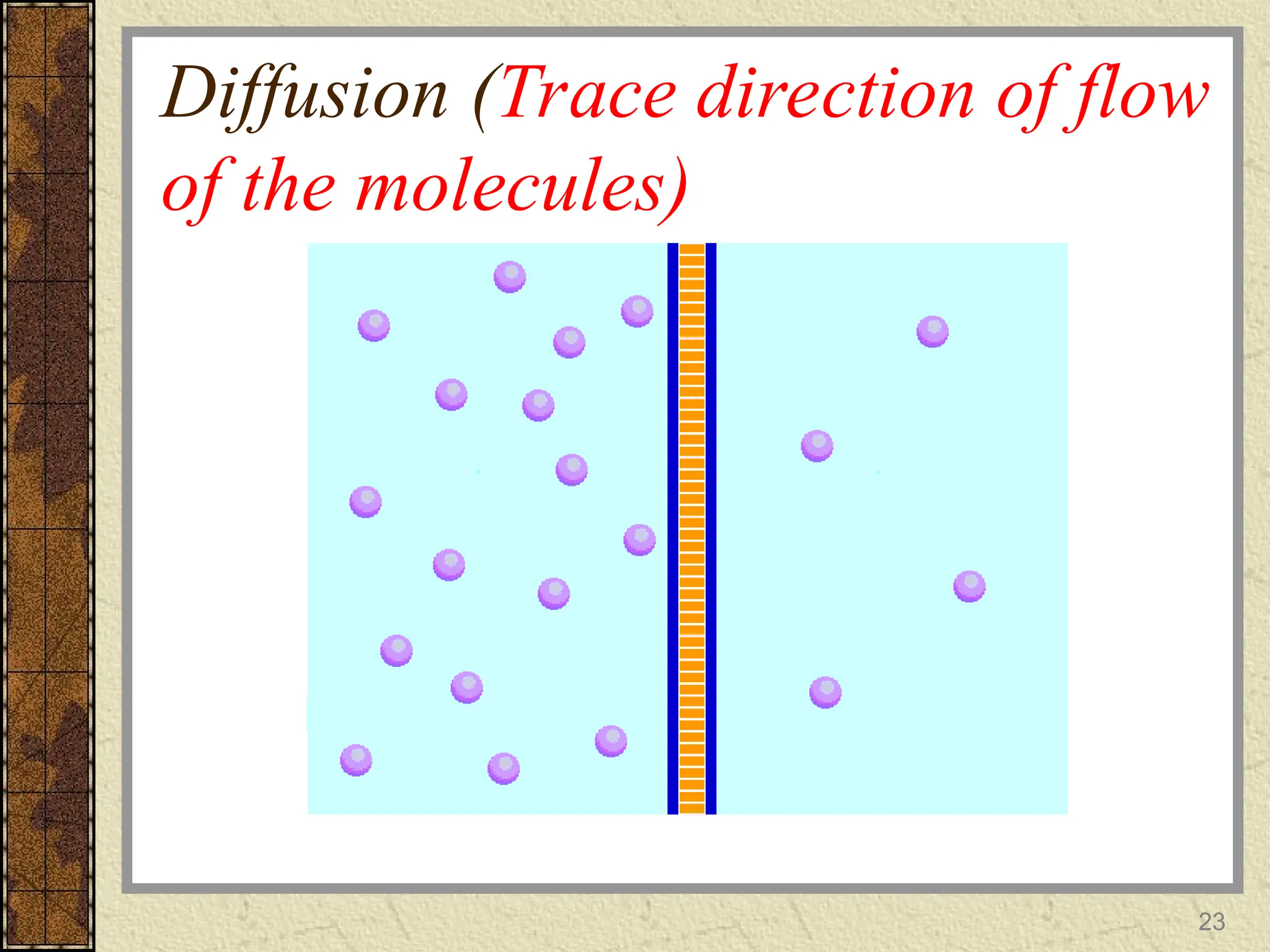
DIFFUSION
Movement of molecules from regions of high
concentration to regions of low
concentration
20
21.
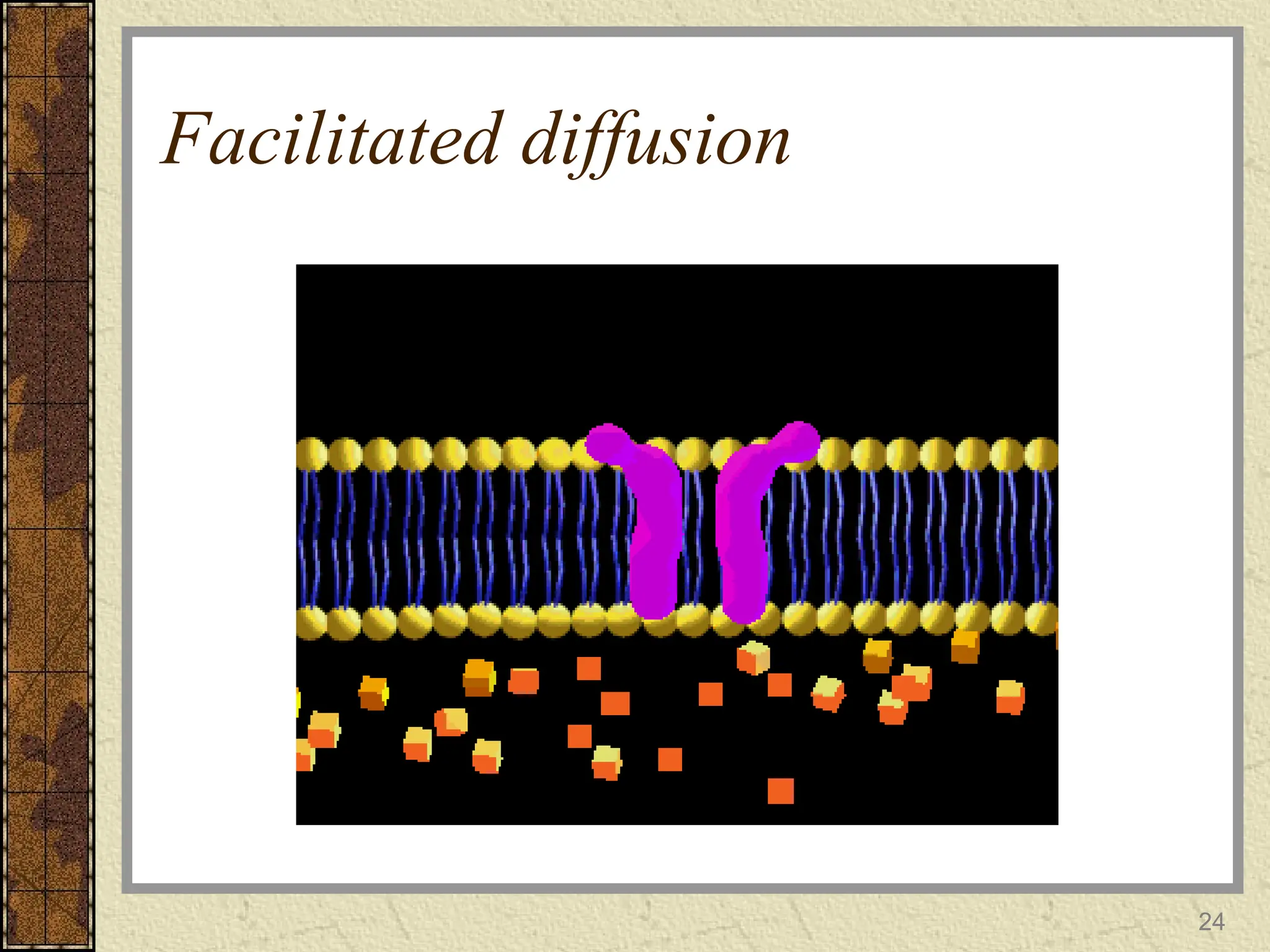
Reading assignment CTs
FACILITATEDDIFFUSION
moving a substance using a carrier from
outside the cell to the inside
ACTIVE TRANSPORT
Use of energy to move particles against their
gradient
21
Regulation of fluidhomeostasis:
(reading assignment: review
work)
4 mechanisms that regulate fluid homeostasis
• ADH (Antidiuretic hormone) Hormone
that stimulates the kidneys to reabsorb
more water; reducing urine volume
(revisit how changes in blood volume or B/P
influence ADH secretion)
• Thirst Mechanism
This is to do with the driving force for
water intake: what happens when you have
a dry mouth? A lowered B/P?
25
26.
Regulation of fluidhomeostasis
CTs…,
• Aldosterone (hormone that regulates
sodium reabsorption)
(Read in the context of `renin-
angiotensin-aldosterone mechanism)
Low Blood Volume triggers renin
release which catalyzes production of
Angiotensin II which trigger the adrenal
cortex to release aldosterone .
Aldesterone increases reabsorption of
sodium hence fluid retention.
26
27.
Regulation of fluidhomeostasis
CTs
• Sympathetic Nervous System
What is the role of the nervous system
in all of the above mechanisms????
There is a deviation from normal, such
deviations must be detected,
information sent to appropriate centers,
appropriate organs/systems triggered to
respond accordingly to normalize the
deviations
27
28.
Terms to Remember
Isotonic:Fluid with same concentration of
solutes to normal human plasma (implications
if infused into the human body?)
Hypertonic: Fluid with a greater conc. of
solutes to normal human plasma.
(implications if infused into the human body?)
Hypotonic: Fluid with a lesser conc. of
solutes to normal human plasma.
(implications if infused into the human body?)
28
ACID-BASE BALANCE
Maintenance ofhydrogen ion concentration in
the body fluid.
Any substance that can donate free H+ ions to
a solution is called an ACID.
Any substance that can decrease H+ ions in a
solution is a BASE.
Number of H+ ions in any solution is
indicated by means of the pH scale.
30
31.
pH
Is a measurementof the acidity and
alkalinity of blood
Conversely proportion to the number of
hydrogen ions in the blood
The more hydrogen present, the lower the
pH will be (acidic)
The fewer the hydrogen present; the higher
the pH will be (alkalinity)
31
32.
The Blood pH
NormalpH in human arterial blood is 7.35-
7.45
For normal metabolism to take place; the
body must maintain this narrow range all
the time
Significant changes in this blood pH range
interferes with cellular functioning and if
not corrected, can lead to death
32
Regulation of Acid-BaseBalance
in the body
High concentrations of acids & bases
are extremely damaging to the human
cells
Acid-base balance in the body is
regulated by chemical buffer systems
and the physiological buffer systems
( kidneys and lungs)
34
35.
Overview of thebuffer systems
• Delicate mechanisms that help the body to
self regulate acid-base balance in order to
maintain pH within the normal range:
1.The chemical buffer systems (Bicarbonate,
Phosphate and protein buffer systems)
2.The physiological buffer systems
(Respiratory and Renal systems)
35
36.
The Chemical Buffersystems
(self study)
Consists of one or more compounds
that resist changes in pH when strong
acid or a strong base is added
Achieved by binding to hydrogen
ions when pH drops and releasing
them when pH rises
36
37.
The Chemical Buffersystems CTs
The Bicarbonate Buffer system
•Mixture of carbonic acid and Sodium bicarbonate
in the same solution
•Buffers mostly ECF
The Phosphate buffer system
Works nearly identical to the bicarbonate buffer
system
Mixture of HCL and Sodium phosphate
37
38.
The Chemical Buffersystems
CT..,
Protein Buffer system
Involves the proteins in the plasma and in
the cells
PLEASE EXPLORE MORE ON THESE 3
CHEMICAL BUFFER SYSTEMS
38
39.
The physiological buffersystems
The respiratory buffer system
•CO2 is normal by-product of cellular
metabolism
•This CO2 is carried in the blood to the
lungs
•Excess CO2 in the blood combines with
water to form carbonic acid
39
40.
The respiratory buffersystem
cts..,
• The carbonic acid later dissociates to release
the hydrogen ions and Bicarbonate
• The blood pH will therefore change
according to the levels of carbonic acid
• This triggers the respiratory system to either
increase or decrease the rate/depth of
ventilation until the appropriate amount of
CO2 is re-established
40
The respiratory buffersystem
CT..,
Activation of the resp system to
compensate for the imbalance starts
to occur within 1 to 3 minutes
The resp syst compensates for
changes in pH by responding to
changes in CO2 in the blood
42
43.
The renal buffersystem
To maintain the pH of blood within normal
ranges the kidneys excrete or retain
bicarbonate(HCO3)
A decrease in blood pH will cause the
kidneys to retain bicarbonate,(weak base
which will accept the hydrogen ions) and an
increase in pH will cause excretion of
bicarbonate through urine
43
44.
NOTE
Respiratory and renalsystems
together:
•Form the physiological buffer systems
that control pH by regulating amount of
acid or base in the body
•Both act more slowly than chemical
buffer systems
44
45.
Issues of nursingconcern
Fluid, electrolytes & acid-base disorders
45
46.
ALTERED FLUID, ELECTROLYTE
ANDACID-BASE BALANCE
Fluid imbalances
Reflect an increase or decrease in total body
fluid or an altered distribution of body fluids.
2 major alterations:
– Fluid Volume Deficit (Hypovolemia) too little -
Dehydration
– Fluid Volume Excess (Hypervolemia) too much
-Overhydration
46
47.
47
Fluid Deficit
Causes
• Abnormallosses through skin ( sweating),
GIT (Vomiting or Diarrhea) or kidneys
through polyuria
• Decreased intake of fluid
• Bleeding
48.
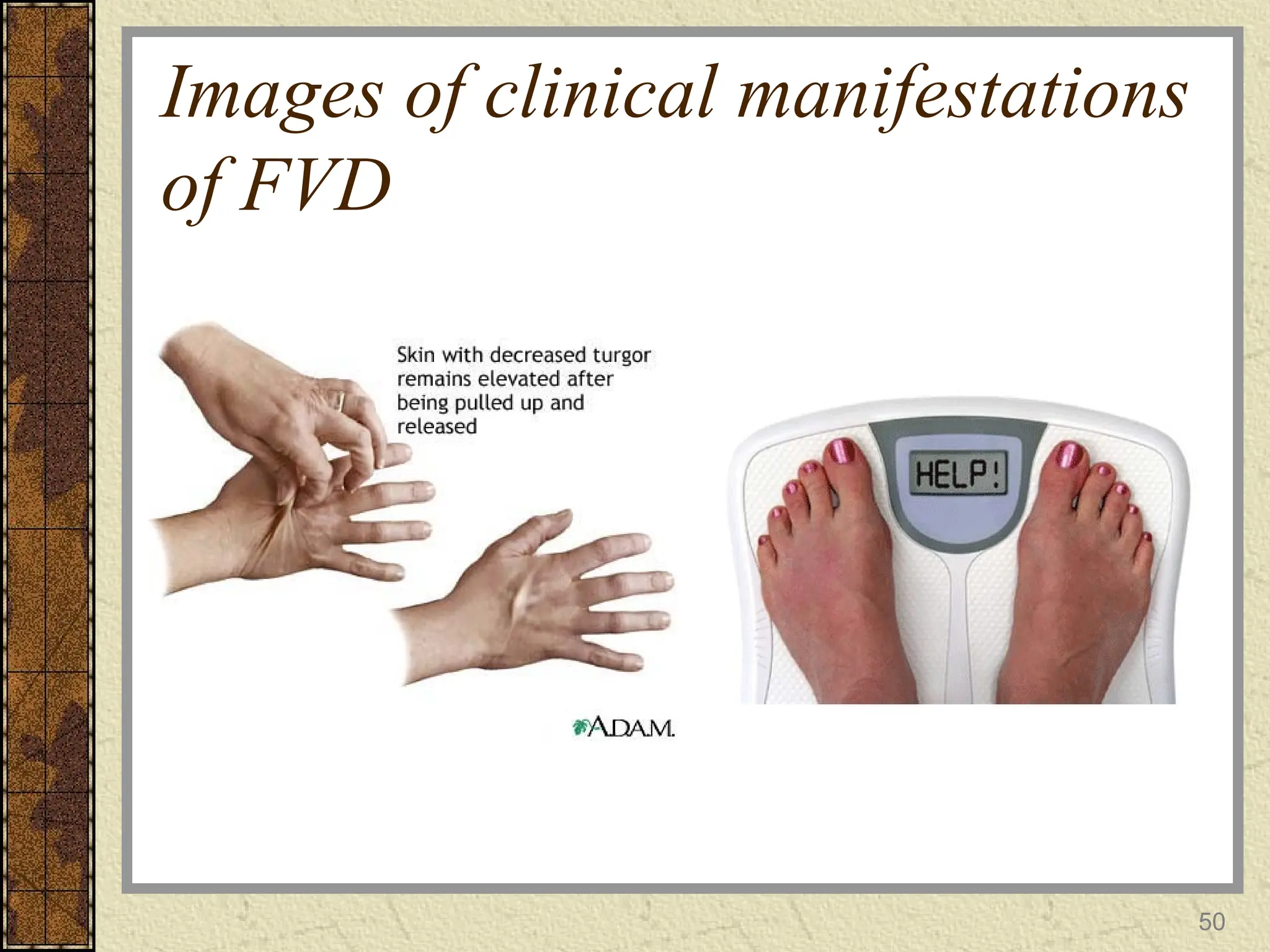
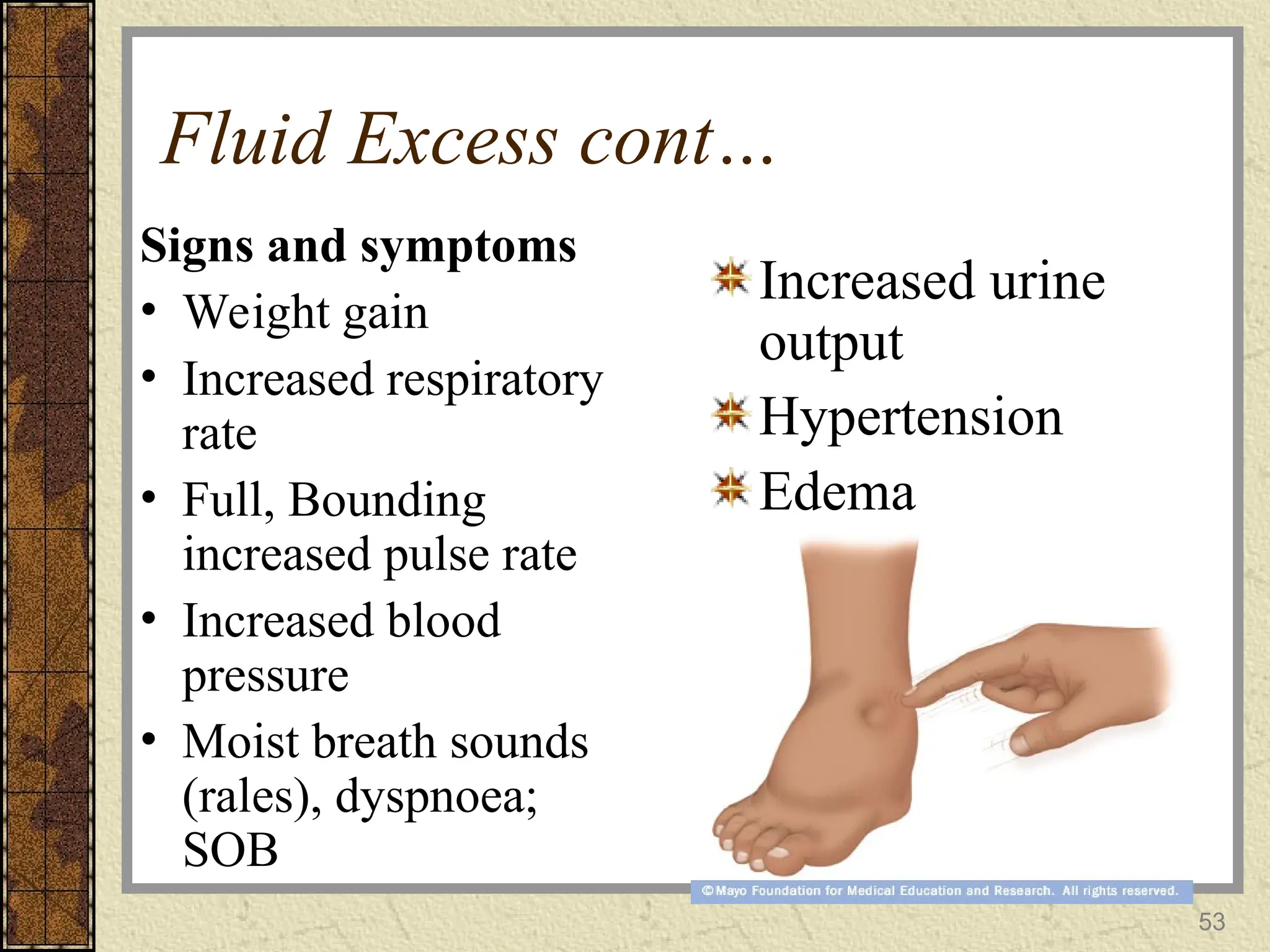
Fluid Deficit cont..
Signsand symptoms
Signs of dehydration
– Decreased skin
turgor
– Sunken eyes
– Lethargy
– Dry mucous
membranes
– Decreased tearing
and salivation
weight loss
Weak and rapid
pulse
Decreased blood
pressure
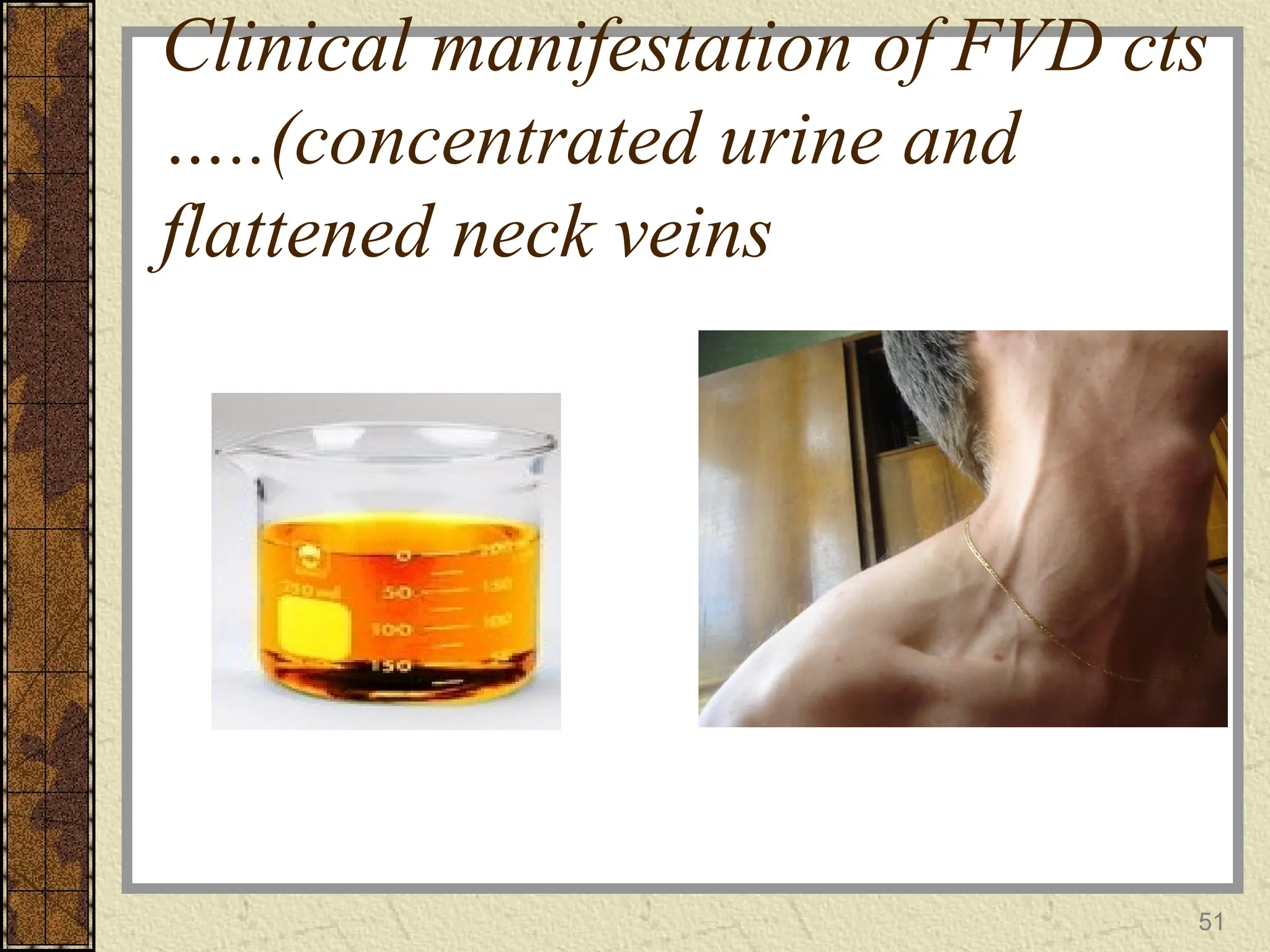
Reduced urine
output and
concentrated
48
49.
Classification of FVD
Mild– 2% of body
weight loss
Moderate – 5% of
body weight loss
Severe – 8% or
more of body
weight loss
49
Sodium
Normal range inplasma 136-145mEq/L
Has most significant osmotic effect in the
extracellular fluid.
Sodium’s major roles act on nerve impulse
conduction, muscle contraction, and
regulation of water movement.
57.
Hypernatremia
Can occur dueto loss of too much water or
addition or retention of too much salt.
Can cause confusion, lethargy, and
eventually seizures and death.
Retention of sodium can occur due to
excessive aldosterone secretion and renal
failure.
58.
Hyponatremia
Can be dueto decreased sodium intake, loss
through vomiting or diarrhea, aldosterone
deficiency, diuretics.
Symptoms include: muscular weakness,
dizziness, headache, tachycardia and shock.
59.
Potassium
Normal range 3.5-5.0mEq/L
Most abundant cation in intracellular space.
Works most on neuromuscular and cardiac
function.
Also helps maintain fluid balance and pH
balance.
60.
K+ imbalances
Hypokalemia- poss.causes: loss due to
vomiting or diarrhea, decreased intake,
aldosterone excess, diuretics, or kidney
disease.
– 1st
symptoms: muscle fatigue and cramps,
arrhythmias, increased urine output
Hyperkalemia- poss. causes: excessive
intake, renal failure, aldosterone deficiency
– Irritability, diarrhoea, nausea/vomiting,
muscle weakness, confusion, numbness
61.
Calcium
Normal range ofunattached Ca2+
in plasma 4.5-5.5
mEq/L. ~Same amount attached to plasma
proteins.
Most calcium in the body is bound with phosphate
in the bones and teeth. In fluids, mostly an
extracellular cation.
Plays important role in blood clotting,
neurotransmitter release, muscle tone, and
excitability of nervous and muscle tissue.
62.
Ca2+
imbalances
Hypocalcemia- poss causes:decreased Ca2+
intake, increased loss, elevated levels of
phospates.
– Numbness and tingling of fingers, hyper reflexes,
increased risk of fractures, muscle cramps, tetany, and
convulsions
Hypercalcemia- poss causes:
hyperparathyroidism, excessive intake of vitamin
D, or some diseases of bone.
– Lethargy, weakness, anorexia, n/v, bone pain, polyuria,
depression, confusion, stupor, and coma
63.
Magnesium
Normal range inplasma 1.3-2.1 mEq/L
54% magnesium deposited in bone matrix.
Mg2+
is the 2nd
most common intracellular
cation.
important in neuromuscular activity, nerve
impulse transmission, myocardial function,
and parathyroid hormone secretion.
63
64.
Mg2+
imbalances
Hypomagnesemia- poss. causes:inadequate
intake or excessive loss in urine and feces.
– Weakness, tetany, delerium, anorexia, nausea,
vomiting, cardiac arrhythmias
Hypermagnesemia- poss. causes: renal failure, or
increased intake such as magnesium containing
antacids or other medications.
– Hypotension, muscular weakness or paralysis, nausea,
vomiting, and altered mental functioning.
65.
pH imbalances
Acidosis- arterialblood pH < 7.35. Poss. causes:
hypoventilation, ketoacidosis, esp diabetic or
alcoholic, renal failure, toxins, very severe
diarrhea.
– if arterial blood pH <7, pt becomes disoriented,
comatose, may die.
Alkalosis- arterial blood pH > 7.45. Poss. causes:
hyperventilation, metabolic alkalosis rare.
– CNS and peripheral nerve overexcitability,
nervousness, muscle spasms, convulsions, and death.
66.
66
Nursing Process –Assessment
Take nursing history
obtain clinical measurements; weight, VS and
I&O
Physical exam
– Assessing skin turgor
– Neuromuscular assessment
Reviewing results of laboratory tests
performed
67.
67
Nursing history
Obtain datafrom the client about:
Current and past medical history
– Reveals conditions that may affect fluid
balances
– Medications like steroids, diuretics and
treatment prescribed like infusions
68.
Nursing history cont…
Fluidand food intake
– What amount and type of fluids, food do you drink each
day?
– Have there been any recent changes in food or fluid
intake?
– Have you experienced any nausea, pain or loss of appetite
that has altered your intake?
Fluid output
– Find out if noticed any recent changes in frequency or
amount of urine output
68
69.
69
Clinical measurements
Daily weight:measurements should be
under standard conditions, i.e. at the same
time each day, wearing the same or similar
clothing, using same scale.
– Each Kg lost or gained is equivalent to one litre
of fluid gained or lost.
VS every 4 hours
70.
70
Clinical measurements cont..
Intakeand output
– Intake and output is recorded on a graphic sheet
which is individualized for each hospital.
– Fluid balance charting allows for careful
monitoring of fluid input and output
– Usu. Measured over a 24hr period
71.
71
Clinical measurements cont..
Guidelinesfor performing intake and output:
It should be performed when:
Fluid intake and urinary output is less than normal
e.g. urine output less than 30mls per hour
Abnormal fluid losses are occurring e.g vomiting,
bleeding
Intravenous therapy is being administered
Patient has medical problems that affect fluid and
electrolyte status
Patient is not physiologically stable e.g. after surgery
72.
72
Monitoring Intake andOutput
– Assess intake and output accurately at scheduled
intervals and evaluate closely for reduced urine
output and for a positive or negative fluid balance on
24 hour calculations
– Urine output is measured every time the patient
voids. It should be transferred into a calibrated
container so that a measurement can be obtained and
recorded
– If patient has foley catheter, collection bag is
emptied and urine is measured at the end of each
shift
73.
73
Clinical measurements cont..
–Any other drainage is also emptied and measured at
the end of each shift
– Oral fluids ingested, feeding delivered via any tube
that enters the body should be measured and recorded
– If patient has intravenous or blood transfusion,
calculate flow rate. Observe for sluggishness or lack
of dripping or dripping too fast so as to ensure that
fluid infuses at the proper rate
– Intake and output should be roughly equal when
balanced after 24hours
74.
74
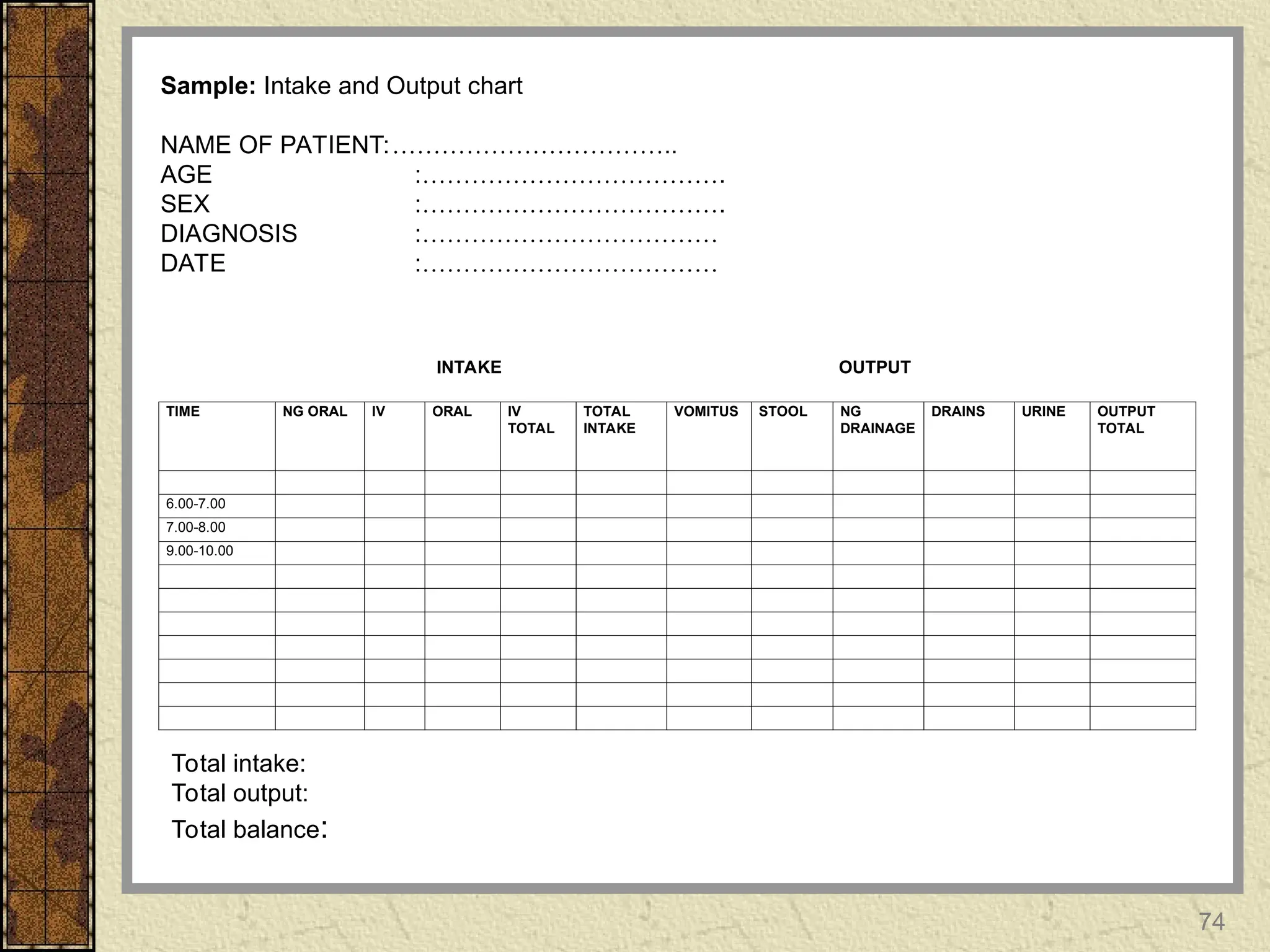
TIME NG ORALIV ORAL IV
TOTAL
TOTAL
INTAKE
VOMITUS STOOL NG
DRAINAGE
DRAINS URINE OUTPUT
TOTAL
6.00-7.00
7.00-8.00
9.00-10.00
Sample: Intake and Output chart
NAME OF PATIENT:……………………………..
AGE :……………………………….
SEX :……………………………….
DIAGNOSIS :………………………………
DATE :………………………………
Total intake:
Total output:
Total balance:
OUTPUT
INTAKE
75.
Clinical measurement Cts…,
Patientsoutput that exceeds intake is at risk
for fluid volume deficit and if intake
exceeds output is at risk for fluid volume
excess
A +ve fluid balance indicates that the input
has exceeded the output
75
76.
Clinical measurement cts..
A–ve fluid balance is the reverse
Note: Adult urinary output is approximately
1500mls – 2000mls per day
Adult intake of fluid is approximately
3,000mls per day
76
77.
77
Physical exam
Focuses onskin, oral cavity, the eyes,
jugular veins, veins of the hands and the
neurologic system
– Integumentary: changes in the skin and mucous
membranes can indicate fluid imbalance
• Skin turgor is best assessed by pinching the area
over the hand, sternum, forehead or inner aspects of
the thigh. In children over the abdominal area or
medial aspects of the thigh:
78.
78
Physical exam cont..
Edema( collection of interstitial fluid in
various parts of the body, i.e. around the
eyes, extremities
– Assessed by pressing a finger firmly over the
sternum or other body surface or boney
prominence for a period of 15 – 30 sec. Upon
removal of finger positive sign is a visible
fingerprint. Use edema scale rates according to
severity
80
Physical exam cont..
Eyes,mouth, lips and tongue key indicators of fluid
volume imbalances: absence of tearing and salivation
(FVD), mucous membrane dry and sticky-mouth dry
and cracked-lips , eyes sunken of puffy
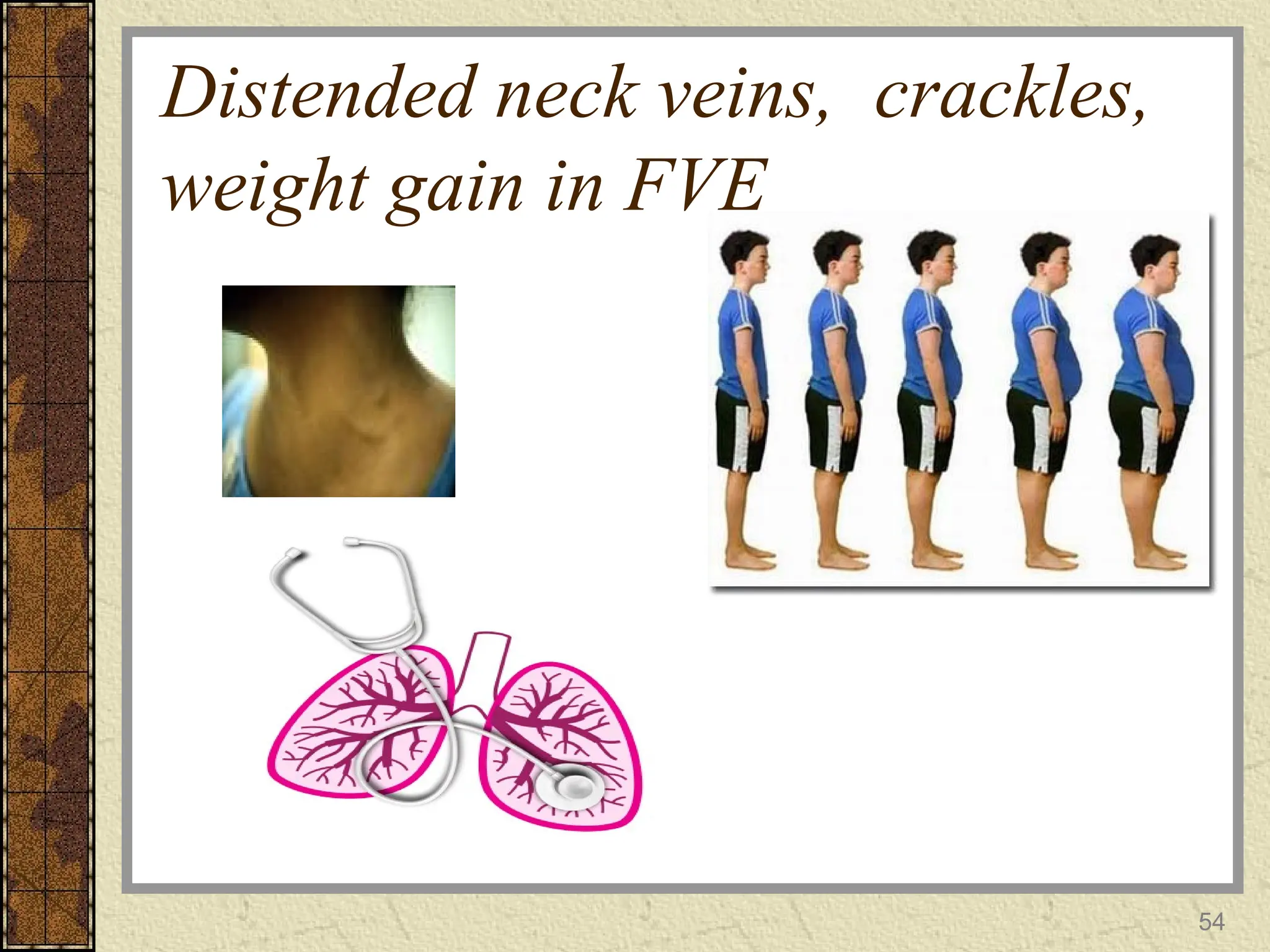
Veins: distention of neck veins accompanies fluid
volume overload. Jugular veins are visible in the
neck.
– To assess place the client with the head elevated to
30º- 45º.
81.
81
Physical exam cont..
Neurologic:Fluid volume changes along
with serum sodium changes affect CNS
cells, resulting in confusion, stupor, seizure
or coma. Assessment of neuromuscular
irritability is particularly important when
imbalances in calcium, magnesium and
sodium are suspected
82.
82
Laboratory Tests
Serum electrolytes
Fullblood count
– Hematocrit (Hct) measures the % of whole blood that is
composed of RBCs. Normal values; males 40%-54%, females
37%- 47%. Increased in FVD and decreased in FVE
– Hgb
Osmolality
– is an indicator of the concentration or number of particles
dissolved in serum and urine. Reported as milliosmols of
solute per kilogram of fluid (mOsm/kg)
83.
83
Laboratory Tests cont..
–Serum osmolality
• Is the measure of the solute concentration of the
blood. The particles included are sodium ions,
glucose and urea (blood urea nitrogen, or BUN)
• Used primary to measure the extent of dehydration.
Normal values are 280 to 300 mOsm/kg. An
increase=FVD; a decrease=FVE
– Urine osmolality
• Is the measure of the solute concentration of urine.
The particles included are nitrogenous wastes
• Normal values are 500 to 800 mOsm/kg. An
increase=FVD; a decrease=FVE
84.
84
Interventions for FluidImbalance
Fluid Deficit - Interventions
– Assess and document amount, colour and
characteristics of vomitus, diarrhea and drainage
from wounds or tubes, vital signs, weight and
skin turgor – accurate assessment enables the
nurse to develop appropriate plans for fluid
replacement therapy
– Oral fluid replacement :
• Facilitating fluid intake
– Explain to the client the reason for the required intake and
the specific amount needed. This gives the client a
rationale for the requirement and promotes compliance
85.
85
Interventions for FluidImbalance
cont…
• Establish a 24 hour plan for ingesting the fluids. E.g. if
2500ml is to be ingested in 24 hours, the plan may
specify 7am-3pm (1500ml); 3pm-11pm (1000ml). Try
to avoid ingestion of large amounts of fluids
immediately before bedtime to prevent the need to
urinate during sleeping hours
• Identify fluids or fluid-like substances the client likes
and make available a variety of those items. Rationale:
intake may be greater when desired fluids are ingested
• Be alert for the cultural implications of food and fluids.
86.
86
Interventions for FluidImbalance
cont…
ORT – special formula
Monitor closely for fluid overload, Monitor vital
signs every 4 hours, weight
Monitor I&O
IV Therapy
Drug Therapy : depends on cause: antiemetic,
antidiarrhea, antibiotic
Oral care,
87.
87
Interventions for FluidImbalance
cont…
Fluid Overload - Interventions
– Assessment of cardiopulmonary, renal, mental,
skin : inspect areas of edema; document location
and degree of edema on a scale of +1 to +4
– Weights, I&O, serum electrolytes,
– VS every 4 hours and prn; I&O
– Drug therapy – osmotic diuretics first, then loop
diuretic such as Lasix
– Diet Therapy – restrict fluid and sodium as specified
by physician
• Explain the reason for the restricted intake and how much
and what type of fluids are permitted orally.
88.
Conclusion
Fluids account fora great proportion of the human
body
About 2/3 of the body is within the cells (functional
units of the body)
Body fluid serves as a universal solvent for a variety
of solutes
Concentration of such varied solutes and the solvent
must be within normal values for healthy life
88
89.
Conclusion
Normal cell functiondepends on physical
and chemical homeostasis of the
surrounding fluids
The fact that on occasion an individual may
not quench for thirst or feel to urinate is a
reflection of the body`s ability for
maintaining it`s fluid, electrolyte and acid
base balances
89
90.
REFERENCES
Craven, R.F. andHirnle, C.J. (2019).
Fundamentals of Nursing: Human Health and
Function. Philadelphia: J.B Lippincolt Co. 5TH
Edition
Kozier, B. et all (2019). Fundamentals of Nursing:
Concepts, Process and Practice. Pearson
Education. Essex.
Marieb, (2013). Human Anatomy and Physiology.
9th
edition Chap 26
90
Editor's Notes
#57 Marathon runner loss of water or too much salt?
If the marathon runner only drinks water, will he have hyper or hyponatremia?



















































![Upper_resp_tract_edited_for_2024_cohort[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/upperresptracteditedfor2024cohort1-250225134620-84a86c8f-thumbnail.jpg?width=640&height=640&fit=bounds)
![MANAGEMNT OF JAUNDICE FOR NURSING STUDENTSt[1].ppt](https://cdn.slidesharecdn.com/ss_thumbnails/jaundiceeditedfor2024cohort1-250318173231-642cf8e8-thumbnail.jpg?width=640&height=640&fit=bounds)
![The Immune system edited for 2024 cohort[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/theimmunesystemeditedfor2024cohort1-250224085036-4b3e6a28-thumbnail.jpg?width=640&height=640&fit=bounds)
![Acute Respiratory Infection Guidelines(ARI)__PRESENTATION[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/aripresentation1-241114171345-63d1411f-thumbnail.jpg?width=640&height=640&fit=bounds)
![Acute Respiratory Infections(ARI)__PRESENTATION[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/aripresentation1-241020112302-e350d353-thumbnail.jpg?width=640&height=640&fit=bounds)
![20971INTRODUCTION_TO_HIV&AIDS for nursing students[1].ppt](https://cdn.slidesharecdn.com/ss_thumbnails/20971introductiontohivaids1-250225134220-578a1188-thumbnail.jpg?width=640&height=640&fit=bounds)
![ASTHMA_IN_CHILDREN for NURSING STUDENT[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/malamuloasthmainchildren1-241125202930-914bc525-thumbnail.jpg?width=640&height=640&fit=bounds)
![Pneumocystis_jirovecii_pneumonia[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/malamulo-pneumocystisjiroveciipneumonia1-241127111242-957cc6eb-thumbnail.jpg?width=640&height=640&fit=bounds)
![management of Chest_trauma for nursing [1].ppt](https://cdn.slidesharecdn.com/ss_thumbnails/malamulochesttrauma1-241127110255-71befbaa-thumbnail.jpg?width=640&height=640&fit=bounds)
![Chest_trauma types and management[1].ppt](https://cdn.slidesharecdn.com/ss_thumbnails/malamulochesttrauma1-241126062258-4b388e87-thumbnail.jpg?width=640&height=640&fit=bounds)


![ECTOPIC_PREGNANCY_disorders of reproductive organs_1_(3)[1].ppt](https://cdn.slidesharecdn.com/ss_thumbnails/ectopicpregnancyupg131-241020092422-a0e8252f-thumbnail.jpg?width=640&height=640&fit=bounds)

![4. EDUCATIONAL PSYCHOLOGY EDITED[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/4-250224085157-3c676047-thumbnail.jpg?width=640&height=640&fit=bounds)
![BURNS assessment and management_GRP_1_PPT[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/burnsgrp1ppt1-241020072724-5845af38-thumbnail.jpg?width=640&height=640&fit=bounds)
![Simulation based learning _Rev[1].ppt JOAB.ppt](https://cdn.slidesharecdn.com/ss_thumbnails/emamatiyafinalrev1-250309104337-a8877e76-thumbnail.jpg?width=640&height=640&fit=bounds)
![INTER-PERSONAL COMMUNICATION IN NURSING [1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/inter-communication1-250309103945-e946794c-thumbnail.jpg?width=640&height=640&fit=bounds)
![Integrated Management -IMNCI_case_management_process[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/imncicasemanagementprocess1-241018200546-4cf422ad-thumbnail.jpg?width=640&height=640&fit=bounds)



















